What will blockchain mean for jobs? One expert says: “30–60% of jobs could be rendered redundant by the simple fact that people are able to share data securely with a common record.”
JobLock
The sharing economy depends on the ability of entrepreneurs to leave big employers with good healthplans. If ACA is repealed and/or individual insurance markets tighten up, the gig economy is going to get slammed. “Job lock” is real; this from HealthAffairs…
Without the ACA, there will be fewer Howards who start their own businesses, resulting in fewer jobs. That’s why anyone who tells you that the ACA is a “job killer” is flat wrong.
What this means – work comp PBMs and payers’ efforts to reduce opioid over-utilization are paying off, and this is excellent news for patients and employers alike.
HOWEVER, with half of all patients receiving at least one script for opioids, we’ve still a long way to go. No vacations folks, now’s the time to keep a relentless focus on reducing opioid usage – especially for patients who’ve been on these drugs for months.
Posted by Joe Paduda on Wednesday, April 5th, 2017 | Comments
Why the President and Congressional Republicans are still trying to do healthcare legislation is truly a puzzle. Unhappy with their initial effort to completely blow up the insurance markets (and their political future), they’ve re-engaged in a pointless effort that is destined to fail – and wound themselves in the process.
Pointless because every concession to win votes from the Freedom Caucus guys costs votes from those slightly more moderate. So, it’s a zero-sum game – win an arch-conservative’s support, lose a less-conservative vote.
perhaps they’re thinking the initial AHCA no-vote debacle wasn’t much of a concern…
To be fair, in the disastrous AHCA non-vote they ONLY lost one of their arms. This time they’re looking to lose more appendages. This is one of those “if you don’t laugh you’ll cry” moments, because ACA does need significant improvement, but – at least for now – improvements are being ignored as politics prevail.
There are a lot of reasons this is political suicide…
The President and Republican candidates committed to keeping coverage for pre-existing conditions. The plan being discussed today would gut this entirely, leaving over a quarter of us without coverage for pre-ex. Ignore claims to the contrary; the combination of changes to what’s covered (essential health benefits) and removal of restrictions on premiums would mean anyone in the individual or small group markets would be subject to medical underwriting (absent state regulations to the contrary).
A close friend and lifelong Republican (including experience working on Capitol Hill) emailed me this morning about this latest “reform the reform” effort using language that would peel the paint off a battleship.
Most Americans now believe the GOP “owns” health reform. A just-published Gallup poll finds 61% of respondents said “any problems with the law moving forward are the responsibility of Trump and Republicans in Congress…”
I think the Freedom Caucus guys understand their ideological purity means millions of Americans will lose insurance coverage – and thus healthcare.
And when they do, every mother, father, aunt, uncle, and grandparent will be incensed beyond measure that their wife/husband/child/grandchild won’t get the care they need.
How that is a winning proposition escapes me, but good for the Freedom Caucus for standing up for what they believe in.
Of course, you need to have legs if you want to stand.
Posted by Joe Paduda on Tuesday, April 4th, 2017 | Comments
Today MCM is honored to bring you a guest post authored by the Sedgwick Institute’s Rick Victor, PhD. Rick is the former CEO of the Workers’ Compensation Research Institute, and a colleague and friend as well.
The post begins below; emphasis was added by MCM.
Trump Immigration Rhetoric and Actions
Risk Higher WC Costs and Slower Return to Work
The Trump immigration actions and rhetoric will significantly worsen the doctor shortage. The Association of American Medical Colleges (AAMC) reports a deficit of 8200 primary care doctors in 2016. It predicts a shortage of nearly 95,000 doctors by 2025. As of 2010, 27% of US physicians were foreign born – 230,000 physicians. Fortunately for US patients, that number has increased each year. Given the large number of baby-boomer physicians who will retire in the next decade, we increasingly rely for our care on foreign born doctors.
The Trump travel ban, rhetoric and recent actions to detain and deport immigrants are creating direct impediments to immigration of needed medical personnel, and a hostile environment for many healthcare workers who consider immigrating to the US for training or jobs. It is in our self-interest to encourage the best and brightest come to the US rather than embracing public policies and rhetoric that repel them.
Seven thousand US physicians were born in the six countries covered by the Trump travel ban. These doctors provide 14 million patient-visits each year. Especially affected are patients in Michigan (1.2 million visits), Ohio (880,000 visits), Pennsylvania (700,000 visits) and West Virginia (210,000). In areas with current doctor shortages, the doctors born in these 6 countries provide 2.3 million patient-visits each year. [The Immigrant Doctors Project used US government data to create a map showing the adverse effects on each local area in the US https://immigrantdoctors.org/.
The negative impact of the Trump travel ban on our healthcare system is much broader than this. First, the rhetoric and initial actions have created substantial uncertainty (and inhospitality) for immigrants from many countries, not just the six listed in the travel ban. The best and the brightest of these have many options other than the US.
Second, both those currently working and training in the US and those considering immigration for training and/or better living conditions are also affected. For those currently training in the US, they wonder if they leave the US to visit family, will they be allowed to returned. When their training is completed, will they be allowed to stay? For those considering training or relocating to the US, they are making a multi-year commitment – mid-course disruption would be very costly to them. The uncertainty created by the recent rhetoric and government actions make the decision to come to the US an increasingly risky one.
Third, we rely heavily on non-physician healthcare workers – 1 in 6 of US healthcare workers are foreign born (nearly 2 million). Forty percent of foreign born healthcare workers are from Asia and the Middle East.
Each year, the US healthcare system depends heavily on immigration to meet the growing demand for healthcare services in the US. Between 2006 and 2010, the number of foreign born US healthcare workers grew from 1.5 million to 1.8 million – adding 300,000 new immigrant healthcare workers.
The US healthcare system relies heavily on foreign born doctors and other healthcare workers. Each year, its reliance grows. The demands on our healthcare system are growing substantially with the aging of the population. Current doctor shortages are predicted to growth dramatically, even if the past patterns of immigration continue. The Trump rhetoric and actions on immigration will impair the flow of healthcare workers immigrating to the US. We will all be worse off as wait times grow and access to needed services becomes more difficult.
Foreign born doctors have choices about where they work. Opponents of single payer models of healthcare financing often cite the longer wait times for patients in single payer systems like Canada and Britain. How ironic if US immigration policies end up reducing wait times in Canada while increasing our wait times.
It’s not that claims with psych issues are inherently much more problematic, or difficult, or costly, or “bad”; but they are when these issues aren’t addressed early and effectively. We’ve long understood that – and the industry has invested tens of millions in predictive analytics, modeling, and early identification.
The challenge has been – what to do about those claims?
Friend and colleague Tom Lynch has developed the only network I’m aware of with providers trained in addressing work comp patients’ psychological issues. Tom’s been in the work comp business for about 40 years, so he knows delivering the right care AND ease of use for adjusters are keys to success for any service provider.
Historically, patients with psych issues aren’t identified early, and the “treatment” that is delivered can take months with little demonstrated progress. There are many reasons for this – but on the provider side, a basic issue is few psych providers know anything about workers’ comp, and many patients are treated for months with little evidence of any substantive progress.
Work Comp Psych Net is currently operating in New Jersey, and delivering remarkable outcomes for patients and payers. I caught up with Tom a while ago to hear more about the problem and how Psych Net addresses psychosocial issues. (I have no financial or legal relationship with Tom or any of his businesses, including Psych Net).
WCPN is comprised of over 50 psychologists covering the entire state trained in workers’ comp who understand the unique issues inherent in comp. These providers use a single electronic scheduling and medical record system which streamlines data collection, Quality Assurance, and reporting. Access and ease of use is critical for both providers and claims staff, a requirement long understood but often poorly addressed.
Today, WCPN is contracted with several payers and actively scheduling patients. To date, on average an initial appointment is scheduled within 27 minutes, with initial reports received by the claims adjuster within 5 days of the visit.
Initial results are promising, with 70% of patients back to work on modified duty within 7 sessions and the other 30% back to work after 11 sessions.
Unlike the typical “let’s get as big a discount as we can” reimbursement model, WCPN’s financial value lies in resolving the claims quickly and for the long term.
“We are asking providers to do more but in a lot less time” is how Tom put it. While WCPN’s per-visit fees may be higher than the deep discount model there are far fewer sessions. “We commit to complete treatment within 12 sessions unless extraordinary issues are presented, then we have to present information to the adjuster as to why it needs to go longer.”
What does this mean for you?
Early identification of patients with psych issues + treatment by work-comp trained providers = much better results for patients – and way lower costs for employers.
Reports indicate the new Administrator, a former lobbyist for the mining industry, will provide “leadership to curtail funding for enforcement, rescind rules under deregulatory orders, and drop defense of regulations facing legal challenges.” The mining industry has been actively applauding initial moves by President Trump to revoke, rescind, or withdraw several regulations and enforcement actions; Pfuelle may have been instrumental in those early actions.
Pfuelle’s past experience includes stints working as a manager in a diamond mining firm in South Africa, labor relations in Liberia’s oil industry, workplace safety officer in the Pakistani ship-breaking association and most recently lobbyist for the Oklahoma natural gas industry.
The White House’s press release noted Pfuelle’s “extensive international experience in a variety of international industries will help America compete with other countries…getting rid of employment-killing regulations will help our economic recovery…”
In an interview after his appointment was announced, Pfuelle was quoted on a number of topics, including return to work. Responding to a reporter’s question about the employer’s role, Pfuelle said:
“OSHA will work to support President Trump’s efforts to make America Great Again wherever we can. If you think about it, a worker injured on the job opens up a job for another worker…so I’m not sure why we want to push employers so hard to rehire injured workers when there are many great Americans who are looking for work…”
In the White House’ announcement of Pfuelle’s appointment, President Trump said: “I’ve known Prelle for decades; he helped me find the best diamond for my first wife. We’ve stayed in close contact, and I was impressed with how he handled the the accident at the Anglo-American Corporation’s Vaal Reefs Mine….while there was some loss of life, he got the mine operating again very quickly…”
According to the reports cited above, first up – after confirmation – is a move to scale back injury reporting requirements.
Speaking about the new electronic reporting requirements Pfuelle opined:
“Employers know when their workers get hurt, and it is their responsibility to make sure they tell us about those situations. But they have a lot of other things that take up a lot of time, so we can’t and shouldn’t expect reporting to be on the top of their list. As long as they let us know in a reasonable time, that’s fine.”
Pfuelle will have to divest his holdings prior to assuming the Administrator position, although, under new rules just released by President Trump’s Office of Ethics, he may choose instead to place them in a “blind trust” directed by his wife Blythe, the daughter of the founder of the Anglo-American Lead Mining company.
According to a Prime Therapeutics study of 15 million commercial insurance claims, short-acting opioid prescriptions dropped over a 15-month period, but utilization of all types of long-acting opioids increased.
In contrast, we work comp Neanderthals have been driving down opioid usage for years.
a few data points…
the percentage of new claims receiving opioids has been decreasing since 2012
the number of opioid scripts per claim has also been dropping
utilization of controlled substances dropped 7 percent in 2014
What accounts for the disparity between workers’ comp and group health?
Work comp payers care deeply about outcomes, function, and return to work. Patients taking opioids are much less likely to return to functionality than those on NSAIDs or no drugs at all.
Some payers have dedicated units focused on chronic pain and prescription drug management. Others rely primarily on their PBMs, but almost all insurers and TPAs have been working this issue for years.
PBMs working in the comp sector dedicate a lot of resources to managing opioids. Investments in analytics, PBM – payer interfaces, staff training, clinical guidelines and the like are costly but drive these results. Staffing – clinicians, pharmacists, data analysts, program managers, highly trained customer service staff – focus on this issue 24/7.
I’m gong to be speaking at this month’s National Heroin and Prescription Drug Abuse Summit on what the real world can learn from workers’ comp. The main takeaway -despite significant regulatory, economic, and legal barriers inherent in workers’ comp, payers and PBMs have made significant progress.
It’s time for the real world to get on board.
What does this mean for you?
We CAN reduce opioid use – it just takes dedication, resources, and persistence.
Posted by Joe Paduda on Friday, March 24th, 2017 | Comments
AHCA has failed, and with it the Republicans’ efforts to repeal ACA.
Despite President Trump’s threats, cajolery, and bribing the Freedom Caucus, the attempt to repeal ACA is, for now and probably for the long term, dead.
Unfortunately, it’s more likely the administration will do everything it can to hamstring ACA – refuse to enforce the mandate, end premium support, defund the federal Exchanges, you name it. In the process, they’ll likely blame the prior president, or Democrats, or whatever. And in so doing, they will hurt businesses, taxpayers, individuals, patients.
What’s most likely is a concerted and persistent effort to defund Medicaid. This will be described as allowing states more flexibility, as refusing to use federal funds for abortions, as reducing the federal deficit, but make no mistake, the real priority is to shrink funding for the poor, elderly, kids, and disabled.
Lest you think that’s harsh, recall that those are precisely the people Medicaid helps. It remains to be seen if Republicans will be successful, or if they will come together and heal the fractures so visible within the party. If they do, they will likely find Democrats willing to work with them, perhaps using the Cassidy Collins bill as a starting point.
There’s been a lot of energy focused on blocking or passing AHCA. Let’s take a few days to let the smoke clear, and then try to get Congress to work together to fix ACA.
Posted by Joe Paduda on Friday, March 24th, 2017 | Comments
I can’t remember a busier and more portentous week in healthcare in the last thirty years.
Last few weeks, in fact. A lot happened in the rest of the world while we (at least us wonks) were obsessing over the latest news from Capitol Hill. Here are some of the highlights
When hospitals are going thru inspections by their accrediting agency, fewer patients die. That’s the finding of a study published in JAMA. (thanks Steve Feinberg MD!) While the percentage reduction was small, the impact was not – if the lower rate prevailed for an entire year across all hospitals, 3,500 fewer Medicare beneficiaries would die – and likely thousands more younger folk. Why?
I’d suggest the Hawthorne Effect is at play: A researcher hypothesized the decrease may be more diligence.
“when docs are being monitored, the focus and attention placed on clinical care goes up. I’d say it was figuring out the diagnosis and matching the treatment correctly, because you’ve been a little more thoughtful.”
Telemedicine prices are going up – from less than $35 per consult in 2009 to around $43 these days. That’s one of the findings from a research report authored by IBISWorld’s Anna Son. More details on this in a future post.
“It takes way too long for adjusters, nurses, and case managers to come to the conclusion that something is going on there. It has been the last thing they look at, and by the time they see it, it’s an iceberg straight ahead and they are about to hit it.”
I’ve been talking about the huge problem of opioids combined with benzos aka sedative hypnotics for some time now. Mitchell Pharmacy Solutions’ Mitch Freeman PharmD. sent me the latest FDA blackbox warning – and reminded me that this is a much bigger issue than that involving combinations of opioids and certain antidepressants.
Finally, good friend and colleague Sandy Blunt of Medata did his usual incredibly competent assessment of a report, and drew some startling – and terrifying – conclusions.
If the WV state avg pop from Census data during this time was about 1.84m and 780m pills were consumed over six years then each and every man, woman, and child in WV statistically consumed 1.36 pills a week –every citizen, every week of the year, for six years without ceasing. If we consider that 20% of the population was under 18 and adjust our data to exclude this group, then each and every man and woman 18 and up in WV had 1.7 pills a week.
Even more disturbing is that this was just (“JUST”) for hydrocodone and oxycodone pills and did not include drugs such as codeine, fentanyl, hydromorphone, meperidine, methadone, or morphine …
Between 2007 and 2012 — when McKesson, Cardinal Health and AmerisourceBergen collectively shipped 423 million pain pills to West Virginia, according to DEA data analyzed by the Gazette-Mail — the companies earned a combined $17 billion in net income.
Over the past four years, the CEOs of McKesson, Cardinal Health and AmerisourceBergen collectively received salaries and other compensation of more than $450 million.
In 2015, McKesson’s CEO collected compensation worth $89 million — more money than what 2,000 West Virginia families combined earned on average. [emphasis added]
McKesson Corp CEO John Hammergren tees off on the 17th hole during the first round of the Pebble Beach National Pro-Am golf tournament in Pebble Beach, California, February 12, 2015. REUTERS/Michael Fiala (UNITED STATES – Tags: BUSINESS SPORT GOLF)
Posted by Joe Paduda on Thursday, March 23rd, 2017 | Comments
Is here at HealthWonkReview thanks to the estimable Louise Norris. She’s picked the most insightful posts from around the web-o-sphere so you don’t have to.
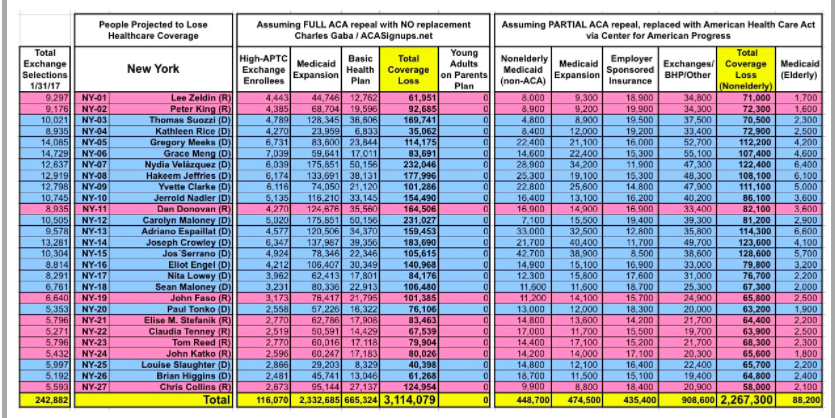
One must-see – Charles Gaba’s analysis of the impact of ACA repeal on Congressional Districts…