Formularies that always allow opioids make no sense. That should be obvious to anyone, and it is to Ms Kellar.
(I’m basing this on an article in today’s WorkCompCentral, which stated:
“A pharmacy formulary is a tool that can be used to address the opioid issue. But it is not the only tool. In fact, Dr. Marcus Dillender, a Ph.D. from W.E. Upjohn Institute for Employment Research, suggests that careful management by insurers and administrators can achieve the same result,”
Sheral Kellar, Esq. is the Director of Louisiana’s Office of Workers’ Compensation Administration; deeply experienced, thoughtful and competent. I met Ms Kellar at CompPharma’s annual meeting last fall when she and several other state regulators spoke about formularies and managing drug usage.
Ms Kellar’s state has the second highest rate of opioid usage among workers comp patients, so she is keenly aware of the issue. She also knows a formulary is NOT a panacea, rather just one tool in the armamentarium.
- Prescription drug monitoring programs that require and facilitate pharmacist and physician participation,
- Strong and well-designed utilization review programs,
- Flexibility for PBMs and payers to customize medication therapy to ensure patients get ready access to appropriate drugs and reduce risks from inappropriate medications,
- Carefully-planned implementation,
- Drug testing, opioid agreements, and addiction/dependency treatment
are all key to the solution.
I hesitate to pick on one issue as THE problem – however any formulary that always allows hydrocodone is not what Louisiana’s workers need. According to WCRI,
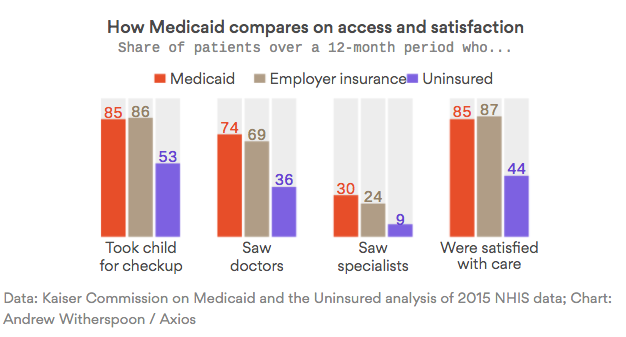
- A higher proportion of injured workers prescribed pain medications in Louisiana (85 percent) received opioids.
- Among study states, LA had the second highest rate of patients taking two or more opioids
- LA had the highest morphine equivalents per claim. – 3540 MEDs, more than double the average.
When you have docs using opioids as first-line pain meds – which clearly is the case in Louisiana, and they prescribe more than twice as much as the average state (which is already too high), and they prescribe more than one opioid most of the time, a formulary that automatically allows docs to prescribe hydrocodone – the most commonly used opioid in LA – is not part of the solution.
What does this mean for you?
Yes, solutions require a multi-pronged approach, but those “prongs” should “first do no harm.”