One of the best conferences of the year is CWCI’s annual get together in Oakland California.
More information is packed into a morning than you’ll find in most multi-day events – and in a more entertaining format – and no one is more informative and entertaining than CWCI’s Alex Swedlow (I’m fortunate indeed to count Alex as a good friend and colleague).
First question – As Alex noted, way back in the pre-Triangle Shirtwaist fire days (no, I wasn’t around then), business claimed 95% of injuries were considered to be the fault of the workers – what is the actual number?
And why do many claims organizations/processes seem to operate as if that statistic is true today?
Okay, back to key takaeaways…
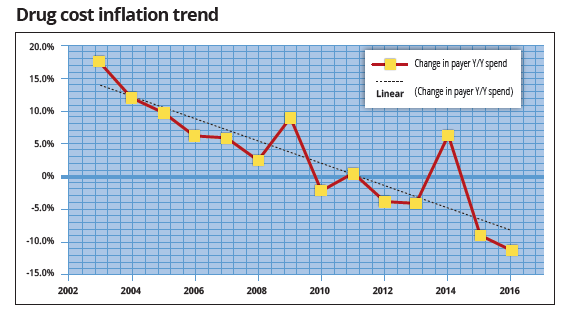
- Average drug spend dropped 34% from 2012 to 2015 – Rx and DME combined amount to 8 percent of total spend of med payments at 24 months after inception
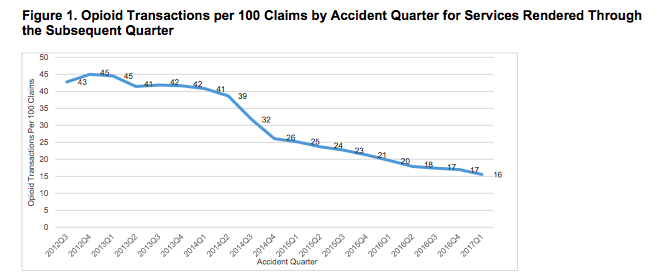
- Opioid spend dropped dramatically, while NSAIDs went up.
- Compared to all claims reported, Cumulative Trauma injuries have increased – a lot – since 2009. CWCI thoroughly debunked the contention by others that CT cases have decreased.
- IMR decisions continue to uphold UR determinations more than nine times out of ten, a rate that’s held steady since 2014.
- UR decisions on compounds are upheld in 99.2 percent of all cases.
- Work comp administrative expenses are higher in California than any other state – by a lot. Part of the answer is the outright abuse of the IMR process by a handful of scummy providers in SoCal…and a couple up north too.
Gary Franklin MD gave a compelling, passionate, and pointed argument that opioid manufacturers are at fault for the disaster that’s killed more than 200,000 of us. Gary never hesitates, never waivers, and is the individual who has done more than anyone else to confront the opioid issue.
More to come next week.