Continue reading Delaney and OneCall Care Management to split
Oct
13
Insight, analysis & opinion from Joe Paduda
Two entries were inadvertently left out of last week’s Health Wonk Review – my apologies!
From Bill Danylik comes this report on a survey indicating perhaps half of large employers are going to be affected by the “Cadillac Tax by 2018. Fine by me; the tax was part of the great compromise reached to fund ACA way back when. It is intended to reduce the favorable tax treatment of benefits, one that subsidizes rich benefit plans.
Posting at the HealthInsurance.org blog, Wendell Potter provides insight into why some states have experienced big increases in individual health insurance premiums. Mr Potter thinks this is due to the similarity between the US health insurance business and the casino industry.
Hmmm, will Native Americans will come to rule health insurance soon?
OK, if you’re off today, enjoy. If not, back to work!
Harvest time is here, and we have a cornucopia of cogitation from contributors for your consideration. (sorry, it’s late…)

The lede
This may be mis-named, as Roy Poses MD’s take on the latest in the ongoing revolving door debacle presents a decidedly unappetizing look at regulatory processes. The candidate nominated to head the FDA has strong ties to the industry he will be regulating. While a superficial review of Robert Califf’s CV doesn’t indicate much of concern, a deeper dive uncovers a board position at a drug company and various and sundry other financial ties.
Dr Poses’ unstinting efforts to teach the rest of us about the far-too-chummy relationships between regulators and regulatees makes him one of our industry’s best.
Implementing Reform
In what may be the umpteen gazillionth effort by the GOPers in the US House of Representatives to do something, anything to kill PPACA, we now have a lawsuit filed by that august body accusing CMS of overstepping its authority re cost-sharing subsidies for exchange enrollees. Attorney Max Horowitz, an expert in the law brings us this tight description of the issue; if you just want to know the basics, click thru.
A huge effort has been underway to automate and integrate health care delivery. Peggy Salvatore shares the latest from the Office of the National Coordinator of Health IT. The ONCHIT announced that it has rolled back Meaningful Use requirements and put in place a 10-year plan for complete nationwide health IT interoperability. These two documents come on the heels of the release of the Federal Health IT Strategic Plan two weeks ago. This is a big deal folks…
Meanwhile, the Colorado version of ACA seems to be moving along albeit with bumps along the way, some of them – shockingly – created by the same folks who continue to try to kill PPACA. Colorado Health Insurance Insider shares what’s happening as health plans set premiums for future years and wonder what happened to the Risk Corridor payments they were promised. Thanks Louise!
The fine folk at HealthAffairs are careful students of all that is payment reform; they direct our attention to limitations in the current shared-savings models employed by Medicare, limitations that means those models don’t work that well for low cost ACOs. Two execs have come up with a creative alternative, one with global risk-adjustment that may address some of the issues with the current model. This is exactly what health reform is supposed to do – get smart people to figure out better ways to do things.
Yay!
Reports of the death of physician private practice may be exaggerated – or at least very, very premature. Jaan Sidorov at Population Health Management provides a very interesting post detailing why and how small physician groups are competing quite well in these days of mega-huge health systems.
My contribution is a piece offering a quick review of a bunch of issues in the healthcare world including the Cadillac tax, premium increases, employee cost sharing, and payer consolidation. All in one easy-to-digest bite!
This next post may cause major indigestion in corporate board suites.
While company executives seem to always escape without any penalty when their companies do bad things, one exec may well get hammered. The top exec at Massey Mining, the company tied to the Upper Big Branch mine disaster is facing trial for his role in the tragedy that killed 29 miners. The question to be addressed involves the level of responsibility a CEO has when things go horribly wrong. WorkCompInsider’s Julie Ferguson includes links to some pretty telling video detailing what CEO Don Blankenship is is accused of.
For post-prandial lethargy sufferers
You know those health plan emails encouraging you to exercise? They may get more serious soon…Hank Stern and friends at InsureBlog are telling us that FitBit may be one way healthplans will find out exactly how many steps you’ve taken. Not to worry; it will be HIPAA compliant.
We’d be remiss if we didn’t give Hank a shout-out; his blog recently was named the #2 Men’s Health Blog. I gotta believe something from Maxim hit the top spot – no other way to keep IB off the top of the podium…and you know how shallow men are!
That’s enough for now. enjoy your Friday, have a ball this weekend, and get out to those Farmer’s Markets!
In 2012, the entire US opioid market was $8.34 billion.
Workers’ comp paid about 17% of that bill.
One of every six opioid dollars was spent by the work comp industry.
That’s a stunning statistic.
Recall that workers’ comp medical expenses account for about 1.5% of total US medical spend. Sure, there’s a lot of pain in comp – but there’s a lot of pain in non-comp diagnoses as well. Chronic non-cancer pain, end-of-life pain treatment, cancer-related pain, acute injuries, surgical recovery, dental procedures can all result in opioid prescriptions.
But few group health patients get opioids for non-skeletal back pain.
What does this mean for you?
We’ve accomplished a good deal in reducing inappropriate prescribing of opioids to comp patients.
But we have very, very far to go. This is NOT the time to rest on our rather meager laurels.
CompPharma, a consortium of workers’ comp pharmacy benefit managers, released the 12th Annual Survey of Prescription Drug Management in Workers’ Comp yesterday. The Survey is an in-depth look at the issue based on telephonic interviews with 21 TPAs, insurers, state funds, and self-insured employers.
This year, we (I’m the author of the study) found that drug costs increased across all respondents. Comparing total 2013 and 2014 drug spend across all respondents, costs climbed 6.4%.
However, that increase was driven by a minority of respondents as only 7 of the 21 saw costs go up.
Looking at inflation another way, we also calculated the average increase for each respondent; trend was essentially flat.
We offer these different metrics to provide readers with as much data as possible so they can draw their own conclusions. One could argue that you have to look at cost changes across an entire industry to really understand what’s happening. Another perspective focuses on individual payers. As the payer’s policyholder base doesn’t change that much from year to year, a payer-specific view is more accurate.
The big question is what is driving drug spend increases. In that, respondents’ views were pretty consistent – physician dispensing, opioids, and compounds. I’d note that the industry has had some pretty good success addressing opioids; PBMs that report on this have all been able to decrease opioid spend over the past couple of years.
Another cost driver, mentioned by a couple respondents, was likely a major contributor: price inflation for generic medications. Fortunately, that has leveled off somewhat of late, although entrepreneurs will continue to look for opportunities to make their fortunes by buying up manufacturers (of little-used drugs) and dramatically increasing prices.
A couple points that bear making.
First, work comp pharmacy is about as different from group health/medicaid/medicare as chalk and cheese. There are:
Second, the PBM industry has done a remarkable job of bringing down the rate of inflation over the last dozen years. Yes, there have been a couple spikes over that time, but ten out of twelve years we have seen a ‘decrease in the rate of increase.”
While premium increases remain at pretty low levels, employees’ share of costs is increasing. In fact, that’s one reason premium increases are as low as they are. Without the higher employee premium contributions, deductibles and copays, premiums would have gone up a couple more points. According to Bloomberg, several factors are contributing:
Consolidation among health plans continues, although there’s little evidence that it will lead to lower costs or better quality.
CEOs from Aetna and Anthem testified before Congress last week, with both touting the benefits of their pending acquisitions of smaller health plans. While it sure looks like the consolidation binge is concentrating power in the hands of a very few health plans, Anthem CEO Joseph Swedish claimed otherwise, stating: “health insurance is flush with competition…The number of health insurers increased by 26% in 2015 with 70 new entrants offering coverage.”
Not sure Mr Swedish’s claim accurately portrays the state of competition in health insurance, and the American Hospital Association and AMA certainly think it’s a bad thing. An analysis by the AMA indicates
The combined impact of proposed mergers among four of the nation’s largest health insurance companies would exceed federal antitrust guidelines designed to preserve competition in as many as 97 metropolitan areas within 17 states
While I am VERY skeptical about any analysis by the AMA, I believe that in this case they have a point. As one expert notes:
I’m aware of no peer-reviewed, published analyses that show that insurance mergers, on average, benefit consumers.
What does this mean for you?
Huge changes in the health care system will have far-reaching implications; watch for more battles between big provider groups and big payers, with smaller payers suffering fall out. This “fall out” will take the form of higher medical costs due to lack of bargaining power,
Friend and colleague Bob Wilson has penned a piece essentially dismissing my claim that pay-to-play exists in the work comp services world. Responding to my series and a great column from WorkCompCentral’s Dave DePaolo, Bob said:
my impression is that major, blatant “payola” in workers’ compensation is rare. At least it has not existed within my personal experience.
In fact, my impression has been completely the opposite.
Bob’s a lucky man, fortunate indeed to not have encountered this sleaze.
I do know of several instances where it has occurred, and Dave described one in detail. And I am convinced there’s a lot more of this than the few instances Dave and I have heard of.
The fact that someone doesn’t know about them isn’t a surprise; by their nature they are entirely secret. If and when these transgressions are discovered by the payor, there is no reason for the payor to publicize the finding and every reason to cover it up. Such is the nature of white collar crime.
I’ve had several conversations with vendors after my series of posts where they described veiled and not-so-veiled requests for services, trips, and other consideration from buyers. It’s real, it exists, and the examples I cited are from conversations with individuals with direct knowledge of these events.
Some have asked why I don’t name names. It is NOT my responsibility to do so. The entities paying these bribes are well aware of the practice yet choose to pay. I am not going to pit my meager resources against those of corporations with hundreds of millions in revenue and legions of lawyers at their beck and call.
That’s part of my disagreement with Bob’s column. The other is that his piece doesn’t address the far more common practice of corporate pay-to-play.
Bob didn’t address the TPA industry’s common practice of charging fees to service companies to do business. That is ubiquitous, and was the subject of a rather contentious debate between Sedgwick CEO Dave North and I at the NWCDC several years ago. At the end of that debate, Mr North a) said Sedgwick doesn’t take much in the way of fees from vendors and b) agreed to share all his vendor contracts with his customers.
I lauded Mr North from the stage and in a blog post for his willingness to publicly offer to share those contracts with customers. I don’t know that any contracts have been shared or any fee-sharing arrangements acknowledged. I certainly haven’t heard about any such disclosure.
To be clear, I’d reiterate a key point made in one of my pay-to-play posts:
What’s not fine is not disclosing the fee-splitting arrangements between the TPA and service providers. Actually, let me refine that – what’s not fine is telling employers no such splitting occurs when it does. Some TPAs tell their customers that they get paid by vendors, and aren’t going to disclose those payments. Again, that’s OK – employers know they are paying “extra” to the TPA for claims and related services, and they know they won’t find out how much “extra” that is. Caveat emptor.
Based on his experience, Bob notes “Are we rife with corruption, with executives on the take and intentional efforts to defraud millions?
Of course not. ”
I suppose it depends on how you define “corruption” and “intentional efforts”.
What does this mean for you?
Employers, are you absolutely, positively, 100 percent certain you know what you are paying for claim-related services?
Courtesy of good friend and esteemed colleague Alex Swedlow of CWCI, I give you the new diagnoses you do not want to appear on your medical chart.
(For a serious review of ICD-10 and workers comp, click here for CWCI’s analysis)
First up, the tragic Y93.D1: Accident While Knitting or Crocheting. Note, needlepoint and lace-making are separate and, well, distinct. One wonders what kind of injury…burnt lip from ingesting overly hot Earl Gray?
Known colloquially as the “Lincoln Diagnosis”, I give you Y92.253: Hurt at the Opera. I know, technically not an opera, but hey, close enough!
Here’s one that doesn’t sound so fun – V97.33: Sucked into Jet Engine. I think I saw something like that in an Indiana Jones movie…but it may have been a propeller, so…never mind!
Among the candidates for most unlikely code ever to appear outside of a blog, I present V91.07: Burn Due to Waterskis on Fire.
From Adam Fein, a candidate for the coveted “developed after coders read The Martian” award – V95.44 (“Spacecraft accident injuring occupant”)
Then there’s this, which makes one wonder if even the ICD-10 coding geniuses thought there could be a sequel – W56.22: Struck by Orca, Initial Encounter.
From there to something that we kinda sorta always knew in the back of our heads was definitely a medical problem, but now we KNOW it ’cause there’s an actual code! Z63.1: Problems in Relationship with In-Laws.
Our oldest daughter is getting married next summer…I’m hoping this isn’t prescience…
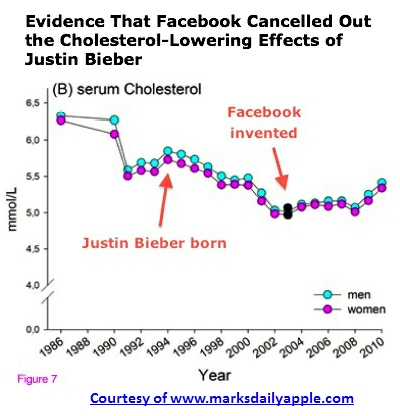
There’s a big difference between “causation” and “correlation”. Just because A is around when B happens does not mean A causes B. It could be that A’s friend C is actually the instigator, and A and C happen to hang out together a lot. Or let’s say B is graffiti at the subway. A can only get out of school on Saturdays which is the only day B occurs because that’s when the graffiti school has their practical exercises.
Or, to be a bit more complex, when Justin Bieber was born, cholesterol scores began to decrease. Until, that is, Facebook was invented, which reversed the decrease, thereby proving the Beebs is not as powerful as Facebook!
Did you know that the more mozzarella consumed in the US, the more civil engineering degrees that are awarded?
Did you know that the age of Miss America strongly correlates with the number of murders by steam, hot objects, or hot vapours?
And the more the US spends on science research, the higher the number of suicides by suffocation strangulation, or hanging… (damn science!)
For those consumed by marriage in Kentucky, know that the marriage rate is closely tied to the frequency of death by falling out of a fishing boat. Perhaps a fishing honeymoon involving moonshine is a time-honored tradition in Kentucky…
Now you know…
But seriously folks, even esteemed medical journals sometimes screw this up – HealthNewsReview highlighted one such faux pas last week in the British Medical Journal of all places.
According to HNR, a BMJ piece about SSRIs and crime stated:
‘Use of selective serotonin reuptake inhibitors (SSRIs) increases the rate of violent crime among young adults.’
The piece SHOULD have said “there is a correlation between SSRIs and an increased risk of violent crime among young adults.”
See the difference? A statistical correlation does not mean one causes the other. In fact, it could be that violent youths are more likely to be prescribed SSRIs, or the crimes studied were committed in an area where psychiatrists prescribe SSRIs a lot more often than in other areas, or any one of dozens of other reasons.
I bring this to your attention, dear reader, because there’s far too much sloppy reporting out there that confuses correlation with causation, often by folks that should know better.
What does this mean for you?
Think critically. Always.
Fall is coming to Colorado’s Front Range, and Louise Norris brings the colors to Health Wonk Review.
Conflicts of interest, 2016 health insurance premiums, preparing for an OSHA audit – that and more await your viewing pleasure!