It’s halftime and time to get a bit of non-football action. Nothing better than a quick trip thru the world of health policy – with Hank Stern as your guide.
Read his edition of Health Wonk Review now!
Insight, analysis & opinion from Joe Paduda
It’s halftime and time to get a bit of non-football action. Nothing better than a quick trip thru the world of health policy – with Hank Stern as your guide.
Read his edition of Health Wonk Review now!
Investors focused on the workers’ comp network and specialty managed care businesses are a bit obsessed with “white space” – the “potential” business, the “opportunity” to capture unmanaged services, to get patients to network providers and thus deliver lower costs to payers and fees for networks/specialty vendors.
During management presentations, potential investors are smitten by the unmanaged care, seeing that as the growth they need to increase the value of the company they’re bidding on.
White space is the term used to describe the volume of services delivered to workers comp patients that are outside the networks used by the employer/insurer. As these “non-network” services aren’t priced at a contracted rate, there is no reduction below the fee schedule or state-set reimbursement rate. No reduction, no savings; no savings, no fee paid to the network vendor.
About 65% of medical services provided to patients are “in-network” – leaving about a third of spend – or around $11 billion in medical costs – unmanaged.
When potential investors look at “unmanaged” services, they see upside, return on investment. What they may well not see is the reality – there’s a reason that space is “white”. Employers, TPAs and insurers have been working since about 1991 to increase network penetration. They’ve tried lots of approaches and generally had pretty good success, especially in states where employers can require patients to go to specific providers or choose from a network.
All the easy stuff has been done – now the real heavy lifting is needed. Increased penetration will come from:
A good way to think about this is that each incremental percent of network penetration takes twice as much work as the previous percent.
That doesn’t mean it isn’t possible. In fact there are some specialty vendors, employers, and insurers making significant progress. These are the careful, thoughtful, analytical companies with very well-developed workflows and a very deep understanding of state regulations, provider behavior, employer limitations, and a lot of people working this every day.
There are others that are stumbling badly – not so much because they don’t know what they are doing, but because actually doing it is really hard, complicated, and requires investment.
And that highlights one of the challenges investors have with work comp. The private equity world is used to automation, stripping people out of processes to improve performance and cut cost. That doesn’t work so well in workers compensation.
What does this mean for you?
If it was easy, it would already have been done.
Too much work and travel last week – actually missed posting three days in a row – my apologies!
Here’s what happened.
In the never-ending saga of California work comp, a recent appeals court ruling found a UR doctor potentially liable for problems associated with terminating a patient’s prescription drugs. The case, King v CompPartners, appears to revolve around the court’s assertion that the UR physician had a patient-doctor relationship with the patient, and thus had a “duty of care”.
If King v CompPartners stands, there could be major implications for California work comp, including significant changes to the entire UR process and landscape. (CompPartners is a subsidiary of MCMC, an HSA consulting client)
Mitchell Pharmacy Solutions acquired PBM Jordan Reses. Mitchell also announced they will re-brand the company’s PBM services as ScriptAdviser. Jordan Reses’ work comp PBM serves a diverse group of employers including school districts, managed care firms, the State of Kansas; it also provides services for the auto PIP program in NJ for Liberty Mutual and other auto insurers. (Mitchell is a member of CompPharma, a PBM consortium; I am president of CompPharma)
After a multi-year hiatus, friend and colleague Bob Wilson finally posted a top ten predictions for work comp . Despite his antediluvian political views, Bob is the most entertaining of the work comp bloggers – myself included.
Final enrollment figures for the public Exchanges are out – Timothy Jost of Health Affairs reports a total of 11.3 million enrollees, 3 million of which were new for 2016. While 35% are under the age of 35, we do NOT know what percentage of this group were dependents. That’s critical, as enrollment among young heads-of-household is key to determine the extent of adverse selectio n.
Tom Barrett of BBG posted on a echocardiogram test a client company paid for; same test, prescribing doc, insurer – two different test providers – 525% difference in cost.
Happy Monday!
Sales and account service people talk about what this or that company says, or wants, or complains about, or what it is basing a buying decision on.
But companies can’t talk – so who, precisely, are these sales & service folks talking about?
This isn’t just an academic question, rather it goes to the heart of customer understanding. The reality is each “client” account is a simply an aggregation of different people, each with their own view of what they want, when they want it, how they want it, and how much it should cost.
And that’s just the high-level stuff.
Successful customer relationships involve a deep understanding of and appreciation for how your company’s services affect the individuals touched by those services. If the senior execs want to see a certain report, then the worker bees have to be able to quickly, easily, consistently, and accurately enter the necessary information.
If your client’s financial folks work best if they get invoices via EDI, then you need to work with their IT folks to set-up a smooth, easy, and fault-free interface and process. Given your client’s IT department is severely under-resourced, and is also your “customer”, you have to figure out how to make this work for them – which may mean you, the vendor, have to do all the work, or pay another vendor to do it for them.
Your business volume depends on your customer’s customers buying services that incorporate your products/services. So, the customer’s marketing and sales folks are also your customers. How can you help them be successful? How does your service/product help them sell more stuff? When problems arise, how will you find out about them and fix them as quickly and completely as possible?
Companies don’t buy and use your services or products, people do. For any product/service “bought” by a company, there are many individuals within that company who will help determine if that sale is a success, if your services are valued, if you get to continue supplying the service or perhaps get to deliver even more.
What does this mean for you?
Look wide and look deep, ask lots of questions and listen really hard – especially to the stuff you may not want to hear.
Some weeks back, the Feds announced they’d reached a settlement with Millennium Health on allegations that drug toxicology firm Millennium Health was involved in illegal practices (my characterization, not theirs).
More recently, Millennium has been working through a reorganization wherein the company’s debtors will assume control of Millennium. This reorg (currently held up by legal wrangling) was driven in large part by a $256 million settlement Millennium agreed to pay to resolve allegations of improprieties.
Note: Millennium is a consulting client, has been for almost four years, and will continue to be a client for the foreseeable future.
A bit more detail on my relationship with Millennium.
I’ve worked very closely with Millennium to design and promote a work comp-specific program. This program – a flat fee covering all drugs and metabolites tested by Millennium, coupled with a payer-specific outreach program and supported by clinical liaison personnel – has been widely accepted by and dramatically slashed drug testing costs for many payers. Everyone I’ve worked with at Millennium – their clinicians, researchers, operations, finance, executive, sales and account management staff – has been professional, highly ethical, and committed to their customers. Over the last four years, I never encountered anything that remotely indicated a possible ethical transgression.
The drug testing program now being considered by Medicare – a flat fee for an entire panel of tests – is what Millennium has been offering work comp payers for over three years.
After extensive research into the allegations and legal wrangling among and between the parties, there appear to be two primary issues described in the DoJ statement referenced above – giving testing cups to physicians, and promoting/allowing physicians to have “standing orders” for drug tests.
Millennium was accused of violating Stark laws by giving docs test cups that the docs would use to collect urine specimens and send those specimens to Millennium for quantitative testing if further testing was required. Millennium was also accused of inappropriately billing Medicare for drug tests by promoting custom “panels” wherein physicians would always request the same panel of drug tests for each payment.
First, the cups – and this is where things get a little confusing. According to Health Law Attorney Blog,
Millennium initiated the practice of entering into “cup agreements” with physicians under which Millennium agreed to provide POCT [point of care testing] cups to physicians free of charge if the physicians agreed: (i) not to bill any insurer for the urine testing service; and, if further testing was required, (ii) to return each test cup to Millennium for lab testing of the urine specimen. If the physicians failed to comply with these requirements, then Millennium would charge them for the price of the cups.
There’s an illuminating discussion of the cup issue here. It looks to me like the key issue is the government’s contention that by giving docs cups with immunoassay test strips attached, Millennium violated Stark laws. If the cups did NOT have those test strips, this would not have been an issue. I’m not clear as to how MH could have violated the Stark laws if the docs did not bill any payer for those cups and thus did not receive any remuneration, but it is clear that this was indeed a violation. As the above-reference Blog notes:
quoting the government here – “whenever a laboratory offers or gives to a source of referrals anything of value not paid for at fair market value, the inference may be made that the thing of value is offered to induce the referral of business.” With that statement, the government clarifies its position that the fact the physician does not bill for the item or service does not, by itself, negate this inference.
So, just giving the cups away, even while requiring the docs to not bill for them, was a violation.
Now, the panels. Drug test are supposed to be specific to a patient; the allegation against Millennium was that physicians and/or Millennium created custom panels of drugs and metabolites, specific to individual physician, panels that would be tested for every patient. Here’s how the Department of Justice described this:
Millennium caused physicians to order excessive numbers of urine drug tests, in part through the promotion of “custom profiles,” which, instead of being tailored to individual patients, were in effect standing orders that caused physicians to order large number of tests without an individualized assessment of each patient’s needs. [emphasis added]
The DoJ also notes the agreement settles allegations that Millennium inappropriately billed Medicare for genetic testing.
Clearly, these were very significant issues. They have resulted in major changes at Millennium including an overhaul of the Board and significant changes to management and ownership. There’s also a requirement that Millennium operate under a “corporate integrity agreement” overseen by HHS for five years.
The $256 million settlement addresses the Feds’ allegations, and there has been no determination of liability. That said, some may well infer that Millennium’s decision to settle the case and essentially turn the company over to its creditors indicates the company was not confident it would prevail if things progressed to trial.
It’s been an ugly, messy, and at times repugnant story. Here’s hoping the legal wrangling ends soon. In the meantime, I will continue to work with Millennium to help them deliver on their commitments to the work comp industry.
Note: Millennium Health has not provided any information to me regarding this matter other than what is publicly available on their website. Millennium has been aware of my intention to write a post on this topic once the legalities were resolved. MIllennium has not reviewed, seen, edited, or otherwise been involved in this post.
It’s been a very, very eventful year. And 2016 may well be even busier. Before I sign off for 2015, a few wishes for the new year.
Donald Trump oozes back under the rock he crawled out from, aka reality TV. Trump’s puerile comments about bodily fluids and his own “greatness” have dominated what passes for serious political debate in this country. Let’s have a smart, informed, fact-based and objective debate about the role of government, foreign policy, tax policy, the future of health care reform, immigration and voting rights. (yes, I still believe in Santa)
Winter comes to upstate NY. Tomorrow’s temperatures here will hit 70 degrees. No snow yet this winter. The warmest year on record, capped by the warmest December on record. Seeing a pattern here…
America doubles down on tolerance, understanding, and compassion. And rejects ideas, policies, plans, and laws based on ignorance, racism, and a desperate attempt to marginalize anyone who doesn’t look or worship the way “we” do.
Here’s hoping you and yours get to enjoy the last week of the year – and it is happy and merry indeed!
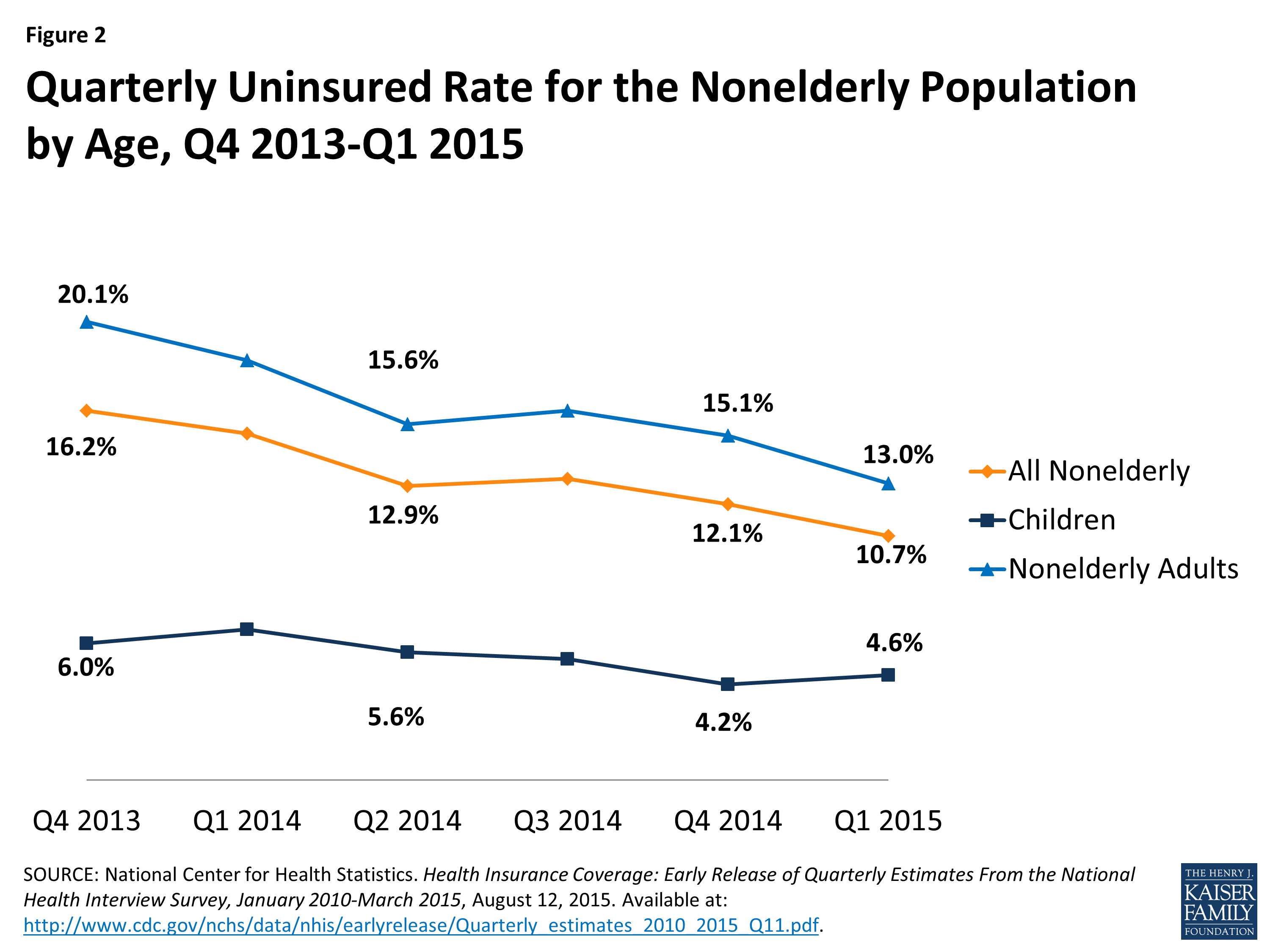
Yesterday we focused on enrollment, and more specifically the change in the number and percentage of eligible Americans covered by health insurance.
In sum, about 9 million more non-elderly folks were insured earlier this year than were at the end of 2013; that means a decrease in the percentage of non-elderlies without insurance from 16.2% of the population to 10.7%.
Today we’ll look at health care costs. One of the ACA’s goals was to reduce future medical costs; to be clear that does NOT mean costs in 2016 will be less than costs today, but rather cost inflation will be lower.
A bit of history is helpful here. I sold health insurance to employers a long time ago; when I could deliver a rate increase below 20%, I felt pretty good. Nowadays, rates are going up in the low teens for most individual coverage – but that’s just part of the picture. Let’s start with total health care costs – because we taxpayers fund Medicare and Medicaid as well as our own coverage.
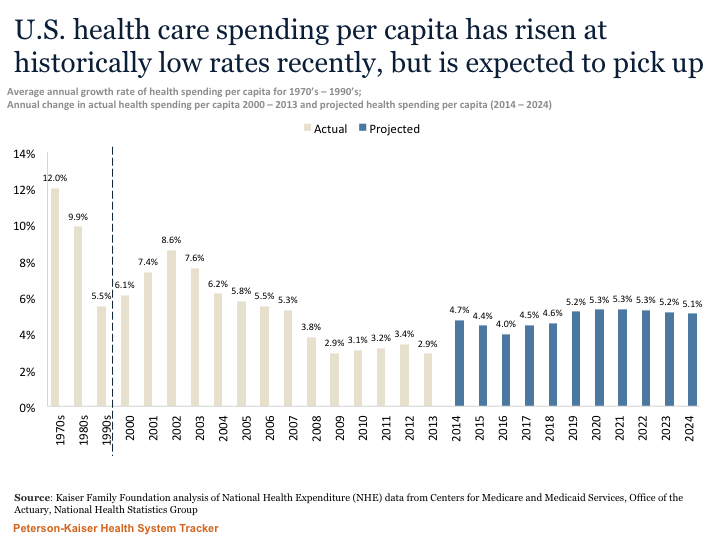
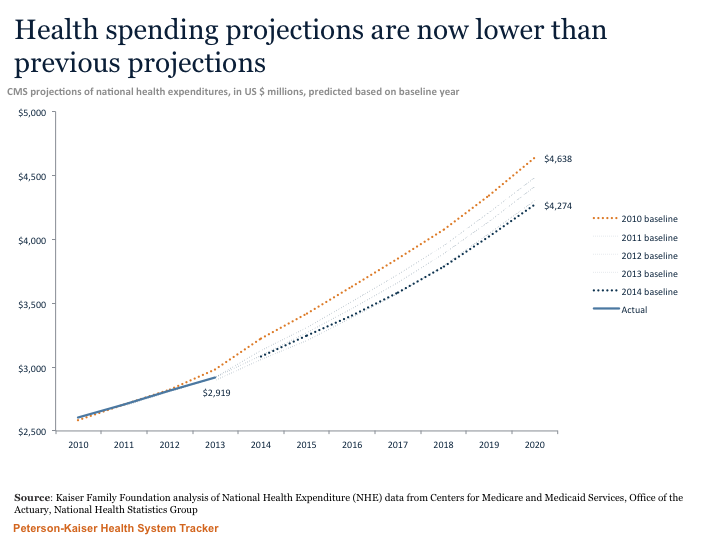
These are projections and as such are just that, however it is useful to compare them to past projections, which had overall medical inflation trending higher than this more recent forecast. (note the figures below are in billions of dollars, not millions)
Now, on to employer and individual costs. Let’s understand that ACA does have SOME impact on costs; added benefits, Exchange distribution, mandated coverage, and the demise of many Co-Ops thanks to the “Rubio Amendment” are repercussions that have yet to be fully felt.
For employers, the latest reports indicate increases of 6.6% (HMO plans) to 9.9% for PPOs for 2016. The primary drivers are prescription drug and hospital pricing; both are up substantially. Notably, Segal’s trend increase predictions have consistently been a couple points higher than the final results.
Finally, I’d note that shopping on the Exchanges can be quite beneficial. We switched from an Excellus Blues Gold plan to a Fidelis Platinum and cut our premiums by $50 a month and out of pocket expenses by several thousand dollars. Better coverage, way better health plan (Excellus screwed up our enrollment, billing, and coverage repeatedly), and less money.
What does this mean for you?
ACA looks to be moderating long-term trend rates overall. Total costs for 2015 are well under prediction and forecasts look good. That said, there are pockets of big increases – some of that due to the lack of competition.
I’d give it a B-.
Let’s start with enrollment…
All in, there’s about 6.5 – 7 million new non-elderly insureds via public and private exchanges to date. The total increase in non-elderly insureds from 2013 to 2014 was just under 9 million (this includes employer-sponsored insurance and governmental programs).
While there’s no completely precise way to get to an accurate number of exchange enrollees, by far the best source for most info is Charles Gaba.
According to the latest estimates, between 32 and 36 million remain uninsured. (the definition used for the latter figure is “at the time of the interview”; as definitions vary, one has to be careful when comparing reports).
Regardless, there’s been a dramatic decrease in the uninsured population since 2010…
Yes, the number of uninsureds remains higher than the original CBO projections. And no, that’s not surprising, given a number of states with a ton of uninsured citizens rejected the Medicaid expansion. According to the CDC,
In Medicaid expansion states, the percentage of those uninsured decreased from 18.4% in 2013 to 13.3% in 2014. In non-expansion states, the percentage uninsured decreased from 22.7% in 2013 to 19.6% in 2014.
About 21% of the 36 million are either undocumented or legal immigrants who’ve been in the US less than 5 years; this population is not eligible for governmental programs or subsidies.
Tomorrow – costs.
In a piece in Insurance Thought Leadership, misleading labeled “Obamacare Expands Into Workers’ Comp”, MaryRose Reaston asserts that
The Affordable Care Act (ACA) was created to expand healthcare coverage. Unfortunately, the act has overstepped its bounds and will dip into the workers’ compensation coffers by requiring mandatory reporting for Medicaid beneficiaries. [emphasis added]
No, ACA has not “overstepped its bounds”. The efforts by states are just that – state-based – and they are allowed/enabled by Federal legislation that is separate and distinct from the ACA. Michael Stack has written an excellent summary of the situation, noting that the federal legislation allowing Medicaid to pursue settlements was part of the Medicaid Secondary Payer Act, which in turn was part of the 2013 Budget Bill..
In fact, I find the attempt to link ACA with state Medicaid recovery activity curious and convoluted. ACA expanded Medicaid – in states agreeing to do so. States remain the primary regulatory bodies for Medicaid. There is nothing in Ms Reaston’s argument that indicates how or by what means ACA encourages Medicaid to pursue workers comp settlements. States that expand or don’t expand Medicaid can decide to pursue settlements – independent of ACA.
Make no mistake, there are clear “winners” here – taxpayers. Any taxpayer should demand Medicaid recover any monies necessary to provide treatment paid for by Medicaid that should have been covered by workers comp.
Hosted by Workers’ Compensation Insider, and stuffed full of the latest and greatest on challenges to the ACA, new news on provider reimbursement, and Roy Poses’ ongoing effort to expose the sleazy side of health care and medical research.
A great way to end the year!