The reason opioid abuse disorder (OAD) is such a huge problem is because no one’s figured out how to a) fix it while b) making a shipload of money.
Sure, there are “solutions” that address bits and pieces including:
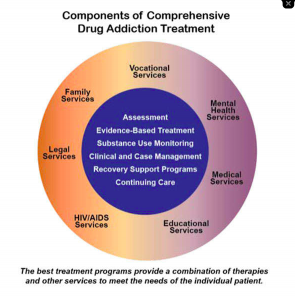
- urine drug testing identifies patients who aren’t taking prescribed drugs and/or are taking other licit or illicit medications;
- Medication Assisted Therapy (MAT) can and does help many wean off opioids without going thru withdrawal;
- inpatient or outpatient detox is essential for some OAD patients;
- physical therapy and exercise is helpful for many; and
- cognitive behavioral therapy (CBT) is essential for many patients.
But many patients require many of these services, while some do fine with one or two.
There is no single silver bullet.
What we aren’t doing is funding community-based treatment facilities and providers. This is essential because OAD is a long-term chronic disease, and patients need follow up and support for years.
The real issue is three-fold – treating OAD usually requires dealing with the patient’s chronic pain as well; OAD is a lifetime disorder; and every patient is different.
The terror of withdrawal coupled with the dread of chronic pain is hugely difficult to overcome. Patients are justifiably terrified of both, and this fear must be addressed throughout the treatment process. This is a long-term process likely involving different treatment modalities delivered by diverse providers.
Some patients respond to MAT, others do not. Some have family support systems, others are pretty much on their own. Some respond to PT and exercise, others are too afraid the effort will trigger a resurgence of pain. And the only way to find out what works for Patient X is to keep trying different approaches, providers, modalities until you find something that works.
No one has cracked the code, come up with a set process, solution or approach that works for most patients. Until someone figures out how to make gazillions fixing people with substance abuse disorder, I don’t expect the nation will make real progress.
That does NOT mean there aren’t real successes happening every day.
California’s State Fund is one of the leaders, delivering remarkable results through a careful, methodical approach.
Here’s the key – OAD can be a lifetime issue. Do not fear this, rather accept it as reality. It’s far easier to throw one’s hands up at the difficulty of it all rather than dig in and get going, but it’s also what led to hundreds of thousands of workers comp patients with OAD.
What does this mean for you?
Those who are in it for the long haul are going to be the difference makers.

I have a less pessimistic view. It makes sense there is no one size fits all solution as we are all individuals. I believe that compassion and the willingness to keep trying are absolutely essential. Also recognizing that as more research is being done, I believe we are going to find chronic opioid misuse leads to changes in the brain that make it difficult (but not impossible) to maintain abstinence. Where I think we will make a difference is in prevention. I would like to see a nationwide requirement for training for chronic pain with alternatives to treatment other than opioids in medical, nursing and pharmacology schools. Additionally a CEU requirement for all medical professionals as a requisite for re-licensure. Nationwide mandatory PBM use and surveillance. Also in the CDC recent meeting they talked about research for Evidence Based approaches to pain treatment for specific diagnoses. Their belief is if the treatment is evidence-based then we should be able to push for parity of treatment. These are all long-term solutions that should stop the pipeline of new patients exposed to unnecessary opioids, and for hopefully treatment, compassion and options for those who find themselves in the Opioid misuse cycle.
Linda
Thanks for the thoughtful observations.
Prevention is well under way and much progress has been made. That’s not the issue here; the issue is that our current corporate medicine ecosystem and the profit motive inherent in american healthcare makes it unlikely the resources we really need to help those already afflicted will be available.
That is the problem.
I too feel this frustration at times. Again, I may be Pollyanna living in a bubble. I have faith in the physicians practicing, the nurses facilitating and the pharmacists dispensing. The vast majority if provided the correct tools WANT to do the right thing. If at the corporate ecosystem level you discuss, you have less faith, then let’s talk about how to increase the public outcry to appeal to their better senses. Keep on researching and applying pressure for parity of care at that level. When listening to the session at the CDC in Atlanta this week I heard total commitment on the part of everyone there.
Thanks Linda. My frustration arises from the total lack of commitment on the governmental level to addressing long-term opioid abuse disorder patients. They are throwing pennies at a problem that requires dollars. For example, community based care requires about $10 billion a year in additional funding. In contrast, the administration has proposed $1 billion and none of that is for community-based care.