Quick take – we don’t know.
Before you read this – don’t freak. Yes this is worse – much worse – than I thought, but panicking and reacting without thinking is NOT helpful.
First, the facts.
- 6,496 people have tested positive for coronavirus; it is in all 50 states
- In the US, 114 of those who tested positive have died.
- We do not know the death rate for three reasons.
- The death rate I (and others) have been quoting is likely misleading – and may be too low
That’s because the number of cases is expanding rapidly but people don’t die immediately. This from the Lancet, based on data from China (as with any early assessment the numbers are rough)
patients who die on any given day were infected much earlier, and thus the denominator of the mortality rate should be the total number of patients infected at the same time as those who died. [emphasis added]
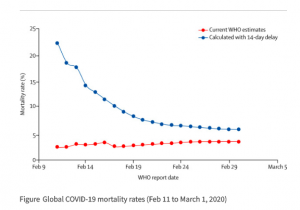
The blue line is the more accurate figure and indicates a death rate of 5.7%.
But…
- Because of the lack of testing (especially early on in China and for far too long in the US), there are a lot of people with mild symptoms or no symptoms that are undiagnosed. Therefore, the denominator (the number on the bottom) is too low. This means the estimated death rate quoted above is likely too high.
- Anecdotally, I’ve heard from healthcare workers that some patients dying of respiratory failure were not tested for coronavirus – thus these deaths aren’t counted as related to COVID-19. Anecdote is NOT data…that said due to the lack of tests, I’m betting the actual number of deaths is higher than reported.
Okay, pretty scary stuff.
What’s scarier is doing stupid stuff – and there is nothing stupider than hoarding toilet paper.
Coronavirus will NOT destroy the supply chain – it will lead to disruptions and delays, but anytime people hoard stuff, that means they won’t need to buy it for a long time. So, while shelves may be empty today, when the supply chain catches up – which it will – there will be lots of pasta, rice, canned food, and yes, TP on those shelves.
What does this mean for you?
Let’s take a lesson from our friends in Italy; be kind and thoughtful, smile at everyone, say hello, and remember we are all in this together.
Oh, and do a lot of takeout and tip generously!

Joe good information to think about. We just won’t know the fatality rate in the short term. You bring up good points above but also consider that only the most sick will get tested. There likely have been and will be many others who have some symptoms but not to the extent that they feel the need to be tested or to go to the hospital. They also believe that it is unlikely COV-19 as they can’t identify a self exposure opportunity. These people will never be counted and this will significantly inflate the fatality rate. Your last point is the take home; be kind and thoughtful, smile at everyone. . . . and reach out via phone or social media who have taken the steps to isolate themselves. If you haven’t done that ask those people if you can be helpful to them buy leaving them needed items, etc.
Good points David – thanks for sharing.
I think we ought to focus on the trends and not the actual numbers. The numerator is grossly understated due to lack of testing, and restrictions/prioritization on testing, and the denominator is most likely understated as well. March 4th there were 158 cases and 11 cases, March 11th there were 1301 cases and 38 deaths, and as of now, there are 6524 cases and 116 deaths. Trends are heading in the right direction, but to your point, there will be a period when this passes that new cases drop but deaths remain flat or increase due to the delay from onset to potential death.
We all need to take a deep breath, not panic, and understand the numerator is going to get way worse, and quickly, before it gets better. Doesn’t necessarily mean it is spreading, but confirming the idea that many, many people already have this virus and testing is finally ramping up 10 fold.
While this is scary, and I have friends and loved ones in the high risk category, I worry for the future that this panic and social distancing may be the new norm. We did not behave this way in 2009 with the H1N1 pandemic was just as serious and deadly, but with 24/7 news, and now social media, it is always in our face and hard to avoid. We tend to have some new health scare about every other year.
Hello Cory – glad to hear you and yours are safe and sound.
thanks for the observations.
I agree – what’s really concerning is the slope of the curve; it’s steepening dramatically every day. I’m not sure things are headed in the right direction as we just don’t have enough credible data on death and infection rates yet.
A needed reminder that math is important – and reading critically is even more so.
best Joe
Good observations – the numbers don’t really mean very much at this point. However, we’re ahead of the curve on prevention and if people are smart and observe sensible precautions, we’re all going to come out the other side with an intact economy and a feeling that this could have been much worse. Stay safe –
always good to hear from you Mike – hoping we are ahead of the curve…I’m not so sure.
Joe, It is great that you bring this to the forefront but I would like to make a couple of points. I am the CEO of CoreChoice and by training, I am a doctor. I also have access to other professionals, most notably an immunologist who is Hopkins trained and an epidemiologist who is Harvard trained. All of these percentages are interesting but we do not know what they are actually percentages of. It appears that approximately 80% of the people who do contract the virus will have no or very little symptoms. This is the most dangerous group because they go along thinking that there is nothing wrong. Yes, people are becoming educated to the fact that we have to maintain our own small spaces but who have we touched on the way to those small spaces is an issue. Another 15% will show the real symptoms of the virus and these are the ones that are easy to figure out. Now many of the patients in the first 95% will resolve with little or no medical care. If a patient has a co-morbidity (hypertension, diabetes, underlying heart disease, COPD or other respiratory impairment, immunosuppression, or other life compromising medical issues), these are the patients who will fall into the category of people who need medical attention. If you then add in the last 5%, these are the patents who are seriously ill and may require hospitalization, intubation, respirators, and ventilators. Then you add in the age factor as it seems that children because they have a higher T Cell count are less affected and younger people (less than age 60) who you would expect to have a higher level of the ability to fight this off, will do better. The important thing to remember is that if patients do not actively show symptoms, they can still transmit. Again, we do not know how these percentages actually apply because we do not know who in the general population are recognizing that they may have the virus and we do not know who is screening and then depending on the result, going for testing. The likelihood is that many of us have already come in contact with someone who either has or has had the virus and we just did not know it. CoreChoice is in the process of setting up a Telehealth platform for patient screening which we hope will be ready shortly. It will staffed by nurses. This is the most important first line of treatment. We hope to have provider offices and urgent care centers on board shortly and if someone does fall into the group that needs to be seen, we will have someplace to refer them or they can contact their own physician. We have also spoken with Quest and while there is availability and Quest just added an east coast processing center for COVID-19, the limit that they currently have is being able to send 15 test kits to providers at a time. We are working with our clients to make this available to as many groups as possible. Screening is the key and no one should be taking this lightly.