Hospitals are drowning in red ink. In many states, workers’ comp is the lifeline.
Privately-insured patients are avoiding hospitals while those facilities have spent huge dollars to buy PPE, make modifications, and ensure they are ready for a COVID19 patient influx.
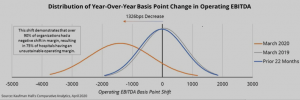
Kaufman Hall provides the graph; the blue curve shows hospital profits pre-COVID, the yellow line reflects COVID. The “0” vertical line is the breakeven point, so the graph indicates the vast majority of hospitals are losing big bucks.
Staff layoffs are all over the news, while research shows the most profitable facilities are getting disproportionally more taxpayer dollars as part of Congress’ aid packages. Rural hospitals are especially hard hit – and this comes after over 150 closed in the last 15 years.
Where are those facilities going to find the $$ they desperately need?
(your picture here)
Just in time, the fine folk at WCRI published a detailed review of outpatient hospital costs and related services. [free to members, there is a charge for non-members] I read the report (yes, the entire thing, minus the super-wonky discussion of statistical methodology). The lede was spot-on:
While the full impact of COVID-19 is currently unclear, this study will also be a useful baseline to monitor the effects on hospital payments.
The analysis is thorough, comprehensive, and easy to follow. Rui Yang PhD and Olesya Fomenko PhD have analyzed 36 states; here are a few key takeaways.
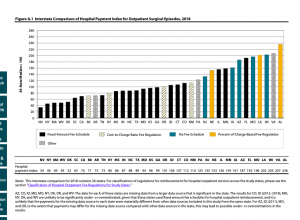
- costs in states without fixed-amount fee schedules are at least 50% higher than in those with fixed-amount reimbursement
- in states with fee schedules, percent of charges fee schedules are the worst offenders [my words not the authors’]
- BUT, there are gaping loopholes in other fee schedule types that allow facilities to maximize reimbursement (looking at you, Florida)
- many states don’t even have fee schedules, which in some cases is just as bad.
What’s a payer to do?
First, identify low cost, high quality facilities and direct your patients to them.
Second, do NOT allow physicians to schedule surgeries in high-cost facilities. The Golden Rule applies – she who has the gold rules, and you are that “she”.
Third, “cost” is the actual cost, NOT the PPO discount. Don’t be fooled – discounts tend to be higher at high-cost facilities.
