What’s missing from the debate about AHCA and ACA is any discussion about what’s making premiums so damn expensive. We are arguing over what we pay, not what we’re paying for.
That makes zero sense.
AHCA makes older folks pay more, and lets younger people pay less for health insurance. But it’s a zero-sum game; all of us are going to pay, we’re just arguing over who pays how much.
That’s not to say ACA was much better at “bending the cost curve”. Most real efforts (excepting Medicare physician reimbursement changes) were taken off the table during the negotiation process, so we were left with ACOs, medical homes, outcomes research, and “death panels” instead of:
- federal drug price negotiation,
- re-importation of meds from Canada,
- requirements that new procedures demonstrate higher efficacy and lower cost,
- stringent controls on medical devices, and
- publication of prices and outcomes by provider.
ACA was – and is – an attempt to get insurers to compete for customers by lowering the cost of care. Some – Centene, Molina, Fidelis, and a few others – are succeeding, but the big commercial plans are mostly failing, resorting to hoary old “cost containment” techniques such as higher deductibles and copays instead of real innovation and effective branding and marketing.
This is especially striking as healthcare outcomes in the US are pretty awful, and research clearly proves spending more on physician care does NOT produce better outcomes. In fact, all credible research indicates the US lags well behind other developed countries in terms of health outcomes.
Link between health spending and life expectancy_ US is an outlier – Our World In Data 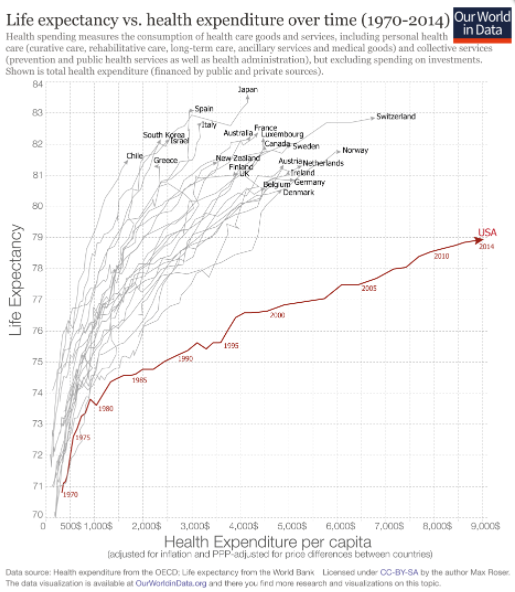
We pay more – a lot more – for health care than other countries.
So, here’s the solution – but one our politicians won’t pursue because they can’t afford to piss off the healthcare lobbying industry.
Cut what we pay for medical care, drugs, facilities and other services, and reduce the volume of services we pay for.
What does this mean for you?
Medical care drives premiums, and if we don’t deal with medical care, we’ll never control what you and I pay for insurance and taxes.

Reducing the volume of services smacks of healthcare rationing and, holy smokes, death panels. …and, as someone who works with primary care, this just sounds like it would exacerbate the problem of access for needed outpatient services such as diagnostic imaging. The pinko in me says that what would really fix the problem is a single payer solution that isn’t reliant on payers making a profit, but that would gut the insurance industry so it would never happen.
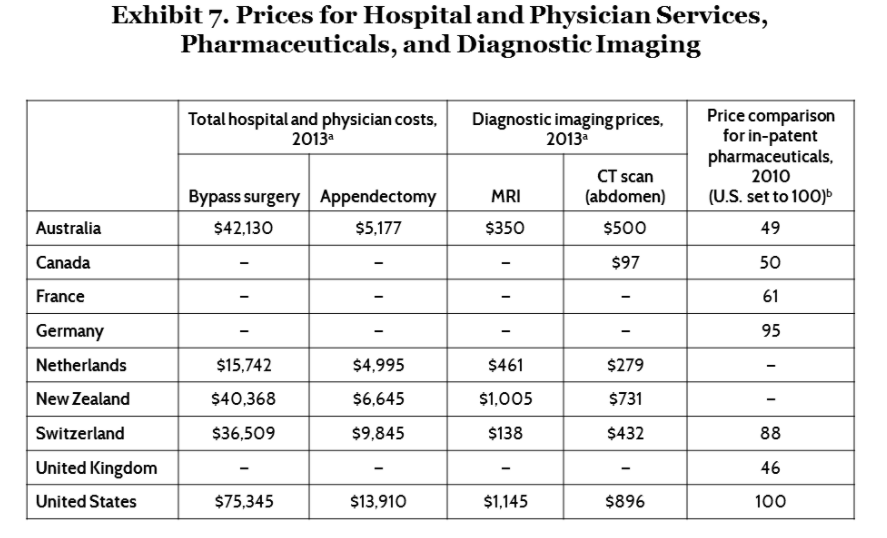
Medical costs in the US are a byproduct of the costs associated with becoming a medical doctor and maintaining a medical license. To more accurately assess the ‘cost’ of a bypass surgery, there should also be a normalizing of the 4 more years of expensive education than in European countries and very high malpractice insurance costs, which are negligible in European countries where medicine is more of a professional trade like engineering or law rather than an advanced educational degree beyond 4 year university education. In the US, if a cardiologist’s patient dies after a bypass surgery, the family sues; in Europe, the family grieves.
S Hensley – welcome to MCM. On what basis do you make the assertion that medical costs are driven by medical education costs? What about pharma, facility, devices, etc.?
also all credible studies I’ve seen do not indicate malpractice or defensive medicine is a significant driver of healthcare costs; if you have sources please share (I’ve posted on this here several times). In addition, med mal does exist in many other OECD countries.
Mr. Paduda – Do the list prices from exhibit 7 reflect gross chargemaster pricing in the US and abroad, or do they include discounts? No doubt there is a significant pricing variation — but I wonder if, like the gross to net rebate situation in pharma, those list prices are inflated…
Hey Mike – first time long time…
source is here
The hospital and physician costs are ” calculated from a database with over 100 million claims that reflect prices negotiated and
paid between thousands of providers and almost a hundred commercial health plans”
the drug prices were “Prices in the U.S. were based on prices negotiated between private health plans and health care providers.
Great article, Joe!
What about regulating the billed charges for healthcare related services?
Perhaps a limit could be placed on billed charges so that they are more closely correlated to the average ACTUAL REIMBURSEMENT for medical services or equipment. For example, there is no reason whatsoever (including the “uncompensated care” argument) why a hospital or other medical provider should charge many times more than what they receive in compensation from Medicare or other payers. Recent transparency efforts under Obama (billed charges vs. Medicare reimbursements) helped but consumers rarely ‘shop’ using the available data.
Sadly, this is a two way street as commercial payers also benefited for YEARS from overly inflated charges. Why? When billed charges are out of reach of the capability of patients to afford then those patients must buy insurance.
Every EOB that we receive after a medical encounter serves as a clever marketing message from the insurance payer: Billed charges = $500, Insurance Payment = $80, Patient Responsibility = $70 The imbedded “marketing’ message”: “Thank God that you had insurance, otherwise, that visit would have cost $500!”
Think about the implications if the provider had only billed $150. In today’s system, the patient might second-guess why they are paying nearly half of the visit cost (re-directing their focus on increasing co-payments and deductibles while premiums continue to increase as well!) or potentially their need for insurance in the first place.
Transparency around the actual cost of medical products and services is the elephant in the room that nobody with ties to the current system has or seemingly ever will touch…politically, a 19% share of GDP guarantees preservation of the status quo as well.
Great post, Joe. Both AHCA and ACA focused on access to coverage. Perhaps if we reduced the cost of care, health insurance premiums might become affordable. I hope your readers can contribute some more cost-savings ideas.
American Exceptionalism rises its head again. We seem to think that we have nothing to learn from our fellow developed countries in the world, such as those on the graph that enjoy better health and far less of their GDP wasted on care. As others have noted, there is a major difference between health and health care. The latter has far more to do with lifestyle and diet.
Obama made a major and politically necessary compromise on day one of the ACA by not attempting to move to a single payer system by expanding Medicare from birth to death. We consume too much care at too high a price. I know many doctors, especially young ones, who work for modest upper middle class salaries or less, and who are in favor of a single payer system and would still go to work for the sort of earnings their colleagues make in other places. It works for those countries that we prefer to vacation in and whose lifestyles and economies we admire. Not perfect but people when polled in those places, even the NHS in the UK, prefer what they have to what they believe we have. The notion that our care system represents some free market ideal is nonsense. When you consume and I pay, and vice versa, that is not free market. There is no price sensitivity or shopping going on, thus we need to regulate and control in some way. I am not optimistic given the ability of the small few to convince the majority to vote against their self-interest, as we are seeing now with the ACA debate, when millions of poorer Trump voters are finally concluding that this is really about returning another 4% of now taxed incomes back to the top 1% of earners. On the other hand, it is quite an amusing show to watch. Lastly the comment on educational costs being a justification is off-base. Student debt is a problem with teachers and social workers. And many doctors have had low cost education or even free, via state schools, military service and the like.
Hi Joe,
You know based on our recent exchange that I fully agree with you on this. I recently read an article (that I unfortunately cannot relocate right now) that mentioned about 10 ideas to bend the cost curve, some of which I had never heard before.
My favorite idea was removing or drastically revising the restrictions on the corporate practice of medicine. The current laws drastically restrict competition. We need market disrupters; with the current laws there will never be a healthcare version of Uber or Amazon, that’s a problem.
Other ideas included: Allow hospitals to turn away non-urgent indigent care (offer tax breaks to providers to provide this type of care), overhaul the FDA drug approval process (could this be farmed out to certified third parties), Increase the number of drugs that can be purchased OTC, incentivize/promote telemedicine, do something to address the overly burdensome HIPAA regs. There were other ideas that I can’t remember.
Admittedly I probably like some of these because they tickle my conservative funny bone so they may not appeal to all MCM readers, but there’s gotta be something we can agree on here. (I hope, maybe?)
Mike – I don’t see these as conservative or otherwise, just intelligent. One big issue is how do we get good healthcare to the poor and those unable to care for themselves? And when it comes to healthcare costs, many Americans are poor indeed, while pharma, providers, and others delivering “care” do very well. When the feds closed many mental hospitals decades ago the number of homeless exploded – but because they don’t vote, they got no help. I just don’t see that decision as right or morally justifiable. Something similar is proposed today.
Joe, Great charts and comments. Lets go one step further. Lets focus on Health! Soundbite: “Healthiest Nation: Watch it happen!” George Anstadt MD FACOEM FACPM
We don’t have to look far to see a place where health care is affordable, look at Canada. The cost of insurance for a family of 4 averaged under $12,000 a year in 2015. I think if you added together the costs of employee & employer paid premiums it would be more per year for most employer-provided plans. Single payer would work if the health care and drug lobby were not so pervasive. Until we get money out of election contributions, we can’t reduce the cost of any consumer benefits. We remain the only industrialized country with a health care problem.
http://www.ctvnews.ca/health/true-cost-of-health-care-to-average-family-is-11k-per-year-report-1.2525114