As of this morning 23,459 US deaths have been attributed to COVID19.
That number is almost certainly too low.
The words “have been attributed” were carefully chosen – note I did NOT write “COVID19 killed 23,459 people” or “23,459 people died of COVID19 or “there were 23,459 COVID19 deaths.”
Briefly, that’s because:
a) patients presenting at a hospital with breathing problems, a fever, and a bad headache are often not tested as COVID19 is assumed;
b) severe COVID cases typically lead to heart attack, Acute or Severe Respiratory Distress Syndrome or other problems, and the cause of death [more on this below] may be attributed to a heart attack/ARDS/SRDS and not to COVID;
c) many hospitalized victims also have other health problems; diabetes, high blood pressure, asthma, COPD, cardiac issues. These co-morbidities greatly increase the risk of death and, absent a positive test for COVID19, may be given as the cause of death; and
d) cause of death (COD) can be a judgment call, and multiple CODs can be reported on the “death certificate”.
Here are the facts.
The CDC finally published guidelines for assigning cause of death for COVID19 earlier this month. Needless to say, a lot of people had died from COVID19 before these guidelines came out, so that’s issue One; Issue Two – as noted above, there can be multiple “causes of death”.
For physicians confronted with a deceased patient, determining and assigning a cause or causes of death is often complicated and uncertain. For example, COVID19 leads to much greater stress on the heart as it tries to pump more blood to get more oxygen out of damaged lungs. According to the CDC, when that old, tired, sick heart gives out:
The immediate cause of death [in this case the heart attack], which is the disease or condition that directly preceded death and is not necessarily the underlying cause of death (UCOD) [in this case COVID19], should be reported on line a. The conditions that led to the immediate cause of death should be reported in a logical sequence in terms of time and etiology below it [on the cause of death statement]. [italics added]
Last week, CDC spokesman Scott Pauley said, “It’s likely that COVID-19 related deaths may not be included on a death certificate [italics added] or COVID-19 might be a factor related to an individual’s death but not the main cause.”
Issue Three – no test, no diagnosis (in some cases) From ABCNews last week
“There is no swabbing of deceased individuals anymore and unless the medical examiner has knowledge of a confirmed coronavirus test, then they aren’t being marked down as having coronavirus,” said [New York City Councilman Mark] Levine, whose committee has oversight for the Office of the Chief Medical Examiner.
Issue Four – A related issue is most of the victims of COVID19 are elderly; older people who contract COVID19 are much more likely to die than younger folk.
Of course, older people have more health problems than younger folks, so there are more “potential” causes of death – cancer, heart disease, stroke, hypertension, COPD, kidney failure and the like. Thus there are more opportunities for the pathologist to attribute non-COVID causes as one of the causes of death – which would further skew the numbers.
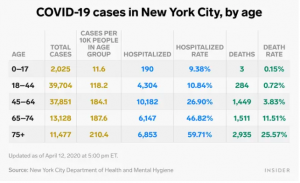
There are compelling data from New York City indicating COVID19 may be involved in many more deaths than have been attributed to the virus;
The FDNY reported a nearly 400 percent increase in “cardiac arrest” home deaths in late March and early April, [emphasis added] a spike that officials say is almost certainly driven by COVID-19, whether they were formally diagnosed or not.
Between March 20 and April 5, the department recorded nearly 2,200 such deaths, versus 450 in the same period last year,
Then there’s the issue (Five, to those still counting) that there are a LOT of “extra” deaths that can’t be directly tied to COVID19 as that specific cause of death, however these “extra deaths” happened during the COVID19 crisis.
This from Judy Melinek M.D., a forensic pathologist:
To quote Dr. Ed Donoghue, a forensic pathology colleague at the Georgia Bureau of Investigation, “No matter how these deaths are currently being attributed, after this pandemic terminates, an excellent approximation of the true fatality rate of COVID-19 deaths can be made by the calculation of the excess mortality for the period. This calculation was very helpful during the 1995 Chicago heat wave. Almost certainly, because of the scarcity of testing and other reasons, we will find that the number of COVID-19 deaths has been grossly underestimated.”
Okay, counterclaims. There are any number of specious claims about rampant over-counting of deaths as COVID; I have yet to see any from any credible source backed by credible data. This is perhaps the best overall discussion of claims that COVID deaths are overcounted; it is thorough and detailed.
Here are just a couple debunked claims…
- “Requirements” that death certificates indicate COVID unless it is a car accident or gunshot.
- Deaths that were “sped up” or “hastened along” – as if all of us aren’t going to die die some day, and anything that kills us isn’t “hastening it along”. Oh, and that’s completely inconsistent with accepted standards for reporting COD.
- Specious and unfounded claims that “if you die of heart disease your death is marked as COVID”
For those interested – The international picture
From the BBC – “it might seem simple enough: if a patient dies while infected with Covid-19, they died of Covid-19.” Perhaps – but they may have died from a car accident, or might have an underlying health condition such as COPD or asthma or heart disease. The UK counts ANYONE who dies and has tested positive for COVID as a COVID death. Even if they died in a car accident.
A related issue – reports from Italy indicate there are a lot more people dying of all causes than usual, and many of those “extra” deaths aren’t attributed to COVID. “Only 12 per cent of death certificates have shown a direct causality from coronavirus,” said the scientific adviser to Italy’s minister of health last week. [source here]
What does this mean for you?
Two things:
We do not KNOW how many deaths are directly or indirectly due to COVID19. But medical experts, physicians, epidemiologists, and medical examiners believe it is significantly higher than the published total.
There are truckloads of BS on the interwebs about COVID; ignore anything not based on solid research from credible people with scientific and/or clinical training and experience.

I suppose you can spin it whatever way you would like to. My research and after speaking with friends that are in the field, says that the numbers are actually high. They aren’t accurate. Many of the folks who died from Coronavirus had other major underlying health conditions. Those that died were tagged corona deaths and in a variety of instances, this is simply not accurate data. The numbers are actually much higher than they should be.
Hello TJ3 – I had responded to you via email, but haven’t heard back. Didn’t want to delay posting your comment, so here it is. Of course, happy to hear back from you if you choose to respond to my email.
first, thanks for the note. I’m not sure what you mean by “spin it”; I cited numerous articles and research documents from credible sources including the CDC, Universities, medical examiners dealing with this every day, and credible journalistic sources in the post. This isn’t “spin”, this is reporting.
You claim the numbers “aren’t accurate”, and that they are “high”, and “much higher than they should be” but don’t provide any backup for your statements.
So, on the one hand I’ve provided a lot of data, credible sources, and quotes from the CDC and medical examiners.
You’ve cited friends and “other research” and provided no backup.
In the meantime, I’d encourage you to click thru the links on the post for more information.
be well – Joe
I’m certainly open to other data and would appreciate it if you could provide that.
” reports from Italy indicate there are a lot more people dying of all causes than usual, …” Can you define ‘a lot’? You are suggesting accuracy and solid sources in your article, which I agree with. So please put some definition behind this statement. Thanks.
Hello Ishtar- thanks for the question.
The numbers you are looking for are in the link on that specific phrase. I did not include specific numbers as the source includes different calculations.
regards Joe
Joe,
Our youngest son, Michael ,is a GI fellow at the Lahey Clinic. he is boarded in Internal Medicine. His chief took him and the other fellows off GI cases a few weeks ago and he is now at the clinic doing internal medicine. He has been assigned a number of cases with renal failure. He believes the COVID-19 virus cases renal problems almost as frequently as pulmonary problems . He is also convinced this virus does lasting damage to many who are infected.
Hello Paul and thanks for the note.
This is a prime example of the key issue here – we are flying blind with no instruments; we just do NOT KNOW what COVID19’s impact will be. If Michael’s experience turns out to be reality, the consequences are broad and deep indeed.
be well – Joe
Then there is the insidious dormancy question: does this virus hide as is seen in shingles cases years after chickenpox? Joe, I do think the numbers are under reported; I think the extent of organ system damage (eg. liver, kidney, cardiovascular) is yet to be known and the collateral damage will be significant, chronic and irreversible; and, post-ventilator survivors will become a unique, problematic cohort. The discussion of residual impact will be akin to watching a Polaroid photo develop.
Always love your provocative composition and its delightful edge.
Stay healthy, stay safe, Stryker
Stryker – always a pleasure to hear from you.
My fear – and it is a rather large one – is COVID19 will persist, and as you note do lasting damage to those most vulnerable.
Be well – Joe
Not to take away from what is being reported here BUT there is increasing scrutiny from reputable medical professionals and others about the numbers and HOW they are being counted and HOW they are being told to count them. If CDC just put out guidelines then they should go back and reclassify the past deaths. Also, why is the regular flu not being handled the same way and where are these numbers? Flu accounts for 24k-60k deaths in the US each year but I see no comparison reporting. Are people no longer getting the flu and only COVID? What about H1N1 comparisons from 2009? Not saying It shouldn’t be taken seriously but there is some major head scratching with regard to the reaction and sense of fear this is causing. I live in a rural area and the reporting has people so scared that I see folks walking down empty rural streets with masks on. Driving alone in their car with masks and gloves on. It’s a little over the top with the fear if that’s what they feel they need to do. The media needs to take a more balanced approach as well and start reporting the 95+% of people who recover or don’t get it.
Here is a credible link: https://m.youtube.com/watch?v=NjjybyJ59Lw&feature=youtu.be
Link to CDC H1N1 (151,700 – 575,400 people died worldwide from the 2009 H1N1 virus infection during the first year)
https://www.cdc.gov/flu/pandemic-resources/h1n1-summary.htm
Mike – thanks for the comment.
I’d suggest there is a lot of fear precisely because we don’t know much about COVID19 and its impact. As you’ll note I’ve written multiple posts attempting to cut thru the noise and describe precisely what we do and do not know about COVID19.
As I noted yesterday, we do NOT know how many people have been infected; as you note there is some evidence many can test positive and be asymptomatic, while others can die relatively quickly – and painfully.
Re the link – sorry, but the interviewee is NOT credible. For example, he asserts that HIV/AIDS is caused not by a virus but by the human immune system over-reacting. That is just nonsense. He is not a medical professional, rather an engineer.
Lastly, we live in NY. This is deadly serious here, and almost everyone takes precautions even in the rural community where our home is.
be well – Joe
Hi Joe. Perhaps, before dismissing this gentlemen with 4 degrees from MIT, you may want to listen to him. I know it sounds foolish that someone who is not a medical professional can provide valid information on immunology but I suggest that ONLY thinking a medical professional can provide valid information is foolish especially when the fact is that the vast majority of medical professionals are trained (or brainwashed) into writing a prescription as the standard of care and have very little understanding of the body’s natural immune system.
My initial thoughts stand: You cannot depending on the numbers being counted or how it’s being counted. WHO and the CDC have been proven wrong and provided bad guidance more than once so referencing them only diminishes the credibility of the writing..
Take 1 1/2 hrs to listen to this and feel free to research his references. I’ve not found one that was incorrect yet.
https://youtu.be/5I46oFxp5L0
Hello Mike – thanks for the note.
The immune response this person was referring to is known as a “cytokine storm”. In the video he insinuated – and repeatedly averred – that the entire physiological issue was due to this immune response.
That is patently not true; many physiological responses to COVID19 e.g. kidney damage, liver problems. fibrosis etc are NOT associated with an immune response but rather the binding of the virus to ACE2 receptors.
I’d suggest that you’re going way out on a limb asserting that this one individual is more credible than pretty much every clinician who is treating patients and almost every mainstream scientist studying COVID19. I don’t understand your assertion that physicians “have very little understanding of the body’s natural immune system.” This is part of basic Anatomy and Physiology, a prereq for medical school admission (I recall studying the immune system when I took A&P in grad school), and curricula in medical school incorporate extensive teaching re the immune system. And every physician treating every disease understands that the treatment must support, not diminish, the body’s immune response. This requires a deep understanding of the immune response.
Of course you’re entitled to your opinion, however it is inconsistent with the views of the the vast majority of scientists and clinicians.
Be well – Joe