Of late there’s been “confusion” in several quarters about the impact of provider networks/PPOs/specialty networks on access to care and outcomes.
These uninformed or willfully ignorant folks claim all manner of bad stuff is due to workers’ comp provider networks – without an iota of evidence to support those assertions.
Let’s pick on the Golden State…
Let’s be clear…actual research shows:
there is NO significant difference in access to care for patients treated within or outside a Medical Provider Network.
This from CWCI’s report…
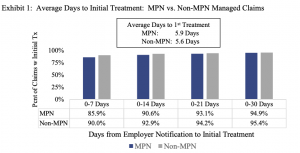
Similarly, there was no significant difference in distance from the patient to provider between MPN and non-MPN patients.
Quoting CWCI…
The latest proximity to care findings also track with results of CWCI’s April 2021 research which found that 99 percent of claims in which treatment was rendered by an MPN provider, and 98 percent of non-MPN claims met the state’s access standards.
What does this mean for you?
Do NOT give any credence to statements similar to: “of course, paying providers less than fee schedule affects access to care” UNLESS they are backed up by real research and not built on a pile of unfounded and unsupported assumptions.

Joe, I hope you take your next column to describe specifically who is confused and what is the confusion about. Quoting a CWCI report from 2022 is likely the most recent data available, however, ‘proximity’ and ‘access’ are not synonymous. CWCI has acknowledged that fact. Dr. Smith’s office may be located within the required distance and is contracted to six different MPNs, but that has nothing to do with her availability to take new patients nor is she required to do so. That problem has become acute in the treatment of mental health. More recently, it has become clear to the Division of Workers Compensation, the medical community, the payor/claims administrator community and the legal community that no one can claim to know what providers are properly contracted to which MPNs. One very large claims administrator, which has access to various PPO and MPN contracts and reimbursement rates for thousands of medical providers, advertises the ability and benefit to stacking those network contract rates so that a customer can be assured of access to the best discount. Also, at least one of the MPN “entities that provide physician services” actively channels injured workers to the providers with which it has the best discounts because its to the “entity’s” financial benefit to do so. Another runs an live online auction of injured workers to physical medicine providers. The lower the bid to provide therapy, the higher the entity’s revenue from that referral. Those transactions and business models are illegal in California. None of the above are assumptions.
Thanks for the note Steve.
It appears you are one of those confused specifically about access and proximity…I don’t understand your statement about proximity and access. The post was specific to access, not proximity (although it did mention proximity in passing). CWCI’s report – and the graph I excerpted from that report – was specific to access, defined as “average initial days to treatment.” I suggest you re-review the post, and CWCI’s report.
Your hypothetical statement regarding “Dr. Smith” is irrelevant as the data shows there is no significant difference between MPN and non-MPN in time to first treatment.
Access to mental health providers is a problem NOT unique to workers’ comp, but one that plagues all healthcare payer types. A shortage of providers is the problem, and that is national.
Couple questions for you. Both reference single, individual entities which as I’m sure you will acknowledge is NOT an indictment of a few, some, many, or all payers or MPNs.
1. Specifically which very large claims administrator is “advertising” the ability to stack rates? Please provide evidence of this practice as it is indeed illegal. How do you know this? What hard evidence do you have of this behavior?
2. Specifically which MPN “channels injured workers to the providers with which it has the best discounts because its to the “entity’s” financial benefit to do so.”? As you note that is illegal. How do you know this? What hard evidence do you have of this behavior?
3. Specifically which entity “runs an(sic) live online auction of injured workers to physical medicine providers” and refers patients based on that entity’s revenue from that referral? That is indeed illegal. How do you know this? What hard evidence do you have of this behavior?
I look forward to your response. If this activity is indeed happening, it should be publicized.
Be well Joe