At some point we’ll have some version of “single payer” healthcare – I predict this will happen within a decade (yes, I know I’m usually wrong on the timing of my predictions, but I’m mostly right on the result).
Whether you’re a rabid libertarian or a totally committed Democratic Socialist, you’ll need to know what Single Payer is.
Single Payer is a catch-all term for universal health insurance coverage. In some cases there isn’t a “single payer” in an entire nation – our neighbor to the north being one example, Switzerland and Germany are two others. In Canada, each Province is it’s own single payer; in the two European countries there are a variety of independent companies that provide health coverage.
That’s how the insurance end of things works. Healthcare providers; hospitals, physicians, therapists are the other side.
The UK may be the best-known example of a “true” single payer system; the government runs the health insurance program and employs most of the healthcare providers.
Between the UK system on one end of the spectrum, and the US “system” on the other, there are a lot of variations.
Here are three examples (borrowed from Dr Lynn Blewett of the University of Minnesota):
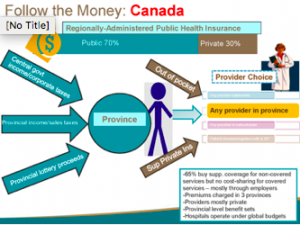
In Canada, there are some variations among provinces in terms of financing and benefits, but these are pretty minor. People can freely choose their providers, there are no deductibles or other cost-sharing provisions, providers are private (not employed by the government), and hospitals operate under a universal budget.
Funding comes from taxes and provincial lottery profits, and about 2/3rds of Canadians buy supplemental private insurance for non-covered services.
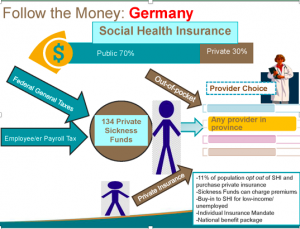
Germany funds its system via general taxes and payroll taxes. There are over a hundred “sickness funds” which are generally equivalent to our health insurers; some charge additional premiums. About a tenth of the population opts out of the national system and buys private insurance coverage. Patients have full choice of the providers they use.
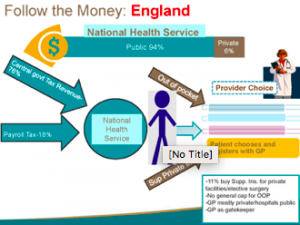
The UK is often held up as the only “pure” single payer system as both providers and the payer are government-based. Funding is via payroll and general taxes. Choice of primary care provider is up to the patient, however PCPs act as gatekeepers to specialty care. Similar to Germany, about a tenth of the population buys supplemental coverage.
California is likely to consider Single Payer after the Democratic candidate for Governor wins the election this fall. Advocates have described their vision for a state-based “single payer” system this way.
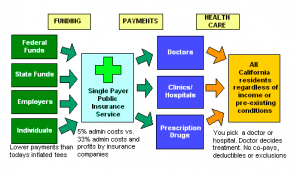
While every system has it’s problems, what is notable is they all deliver better outcomes at significantly lower cost than we have here in the US.
So, when you hear people decrying the ACA, “Obamacare”, or single payer, ask yourself how their “solution” would lower your costs while improving the healthcare you get.
Better yet, ask them…But be prepared for silence.
What does this mean for you?
This will be one of the two most important issues facing us over the next decade. Inform yourself.

Thanks Joe. I hate saying this because I have friends in California but I vote that CA does this and we give it 10-20 years to see if it successful. Same goes with other socialistic program. CA seams to be the testing ground for many socialistic programs and environmental regulations and restrictions. It says a lot when it is predicted that 50% of the middle class will be moving out of CA in the next 5-10 years. High taxes and environmental and liberal policies are making people flee. But I am all for giving this a shot. Just please don’t implement this in the entire US.
Why isn’t our country focusing more on people taking care of themselves? Obesity, Diabetes, Smoking, etc are all preventable diseases. Where is the accountability on people taking care of themselves? I get there are accidents, genetic disorders, etc. but I believe a cheap payment for “catastrophic” injury is very doable. Why not focus on personal accountability and not policies to save everyone from themselves? Why is it this the governments responsibility? I just have a hard time believing the government can run a successful program. I will admit I would be more comfortable if it was state run because I trust our government officials in Utah way more then our federal government but still not a fan of extremely high taxes. It will be interesting (and scary) to see where this all goes.
Thanks again for your time and article. I read them every morning.
HI Spencer – thanks as always for the thoughtful comment.
We agree that people should take better care of themselves – however that butts up against individual freedoms – however dangerous and unhealthy they may be. I’m not sure how we can thread that needle, but I’m all for premiums partially based on modifiable risk factors. Like requiring motorcyclists who ride without helmets to have catastrophic and long term care insurance.
I’d suggest the government does run several very successful programs, including Medicare and Medicaid.
On the government worker side, I think you may be surprised by the quality and commitment on the part of most government workers. As the son of two CIA employees, I am admittedly biased, but many agencies and programs run quite well – except when politicians screw them up or don’t write good legislation to begin with.
I’m not sure a lot of folks will be leaving California – and if they do, many more will move in. Two of our kids moved there, love it, and have no plans to leave. The economy is booming, the state is running a budgetary surplus, and it is home to many of the most successful tech companies in the world.
Thanks for posting Dr. Blewett’s presentation. It was very helpful. Have you seen any studies out there on what the impact would be to the economy under single payor or national health service with regards to job loss and the economy? Example – what would happen to all the folks employed by the many publically traded health insurers? How to unwind publically traded companies? etc. Something I was always wondering about but could not find much info on. Thanks Joe
Jeff – thanks as always for the comment. I have seen data and will refer to it in a later post.
thanks
A couple of comments. I have spent some time in Montreal and London lately and have asked everyone from cab drivers to insurance people about their national healthcare programs. It was hard to find anyone in either city who had good things to say. Canada’s program currently has the longest wait times in the history of their nationalized program. One thing was clear – the national programs are only for the masses. The wealthy in both countries use private health providers and when really ill, often travel to the US for life saving medical services.
I hope for the sake of the worlds population that we don’t abandon our current system of healthcare. While bloated, full of abuse and overly expensive, we nevertheless provide the world with over 90% of advances in medical technology and 95% of drug discovery. I would also hate to see a two tier system like England and Canada where the elites and rich have great healthcare and the 90% deplorables are left with something less.
Hello Tom – thanks for the note.
we too have a split system, with Medicaid for the poor and commercial insurance for the employed. And no insurance for about 20 million of us.
The issue is this – our healthcare is unaffordable. the current system is failing.
is there another alternative? i don’t see one.
If anyone is against single payer, consistency would demand that they be opposed to Medicare and the VA – both of which are single payer, tax-based systems for their respective constituencies. If one does not see the inconsistency of this, I am all ears and look forward to the contortions that will explain convincingly that this does not count. As to the impact on society of a new system – the biggest impact would perhaps be anything that would return about 5% to the GDP assuming that a new system might put the US more at par in terms of national health spending to other nations we admire. As to waiting lists pointed out in Canada, as they say, there are trade-offs in anything. If one really wants to see 18-20% of GDP going to health care vs. 13% and might in essence see several thousand dollars or more in their pocket annually, but has to wait for an MRI – what is the decision here that most would make. It would cost jobs in the health sector. It would mean disruption to aspects of the economy. But we have seen this before in many arenas and will again. Witness the profound impacts that the computer I am typing this on has wrought to any number of jobs.
I agree that a tipping point is getting closer and single payer is seeming less and less a radical idea and that the political will appears to be shifting in that direction. If so, the bigger question is what will it look like and who will be the many losers and the relative winners. Or might folks just try to keep the dollar amount the same and put it in different pockets. There is a physicians group PNHP that is studying and advocating on the issue (PNHP.org).
https://www.healthsystemtracker.org/chart-collection/health-spending-u-s-compare-countries/#item-since-1980-gap-widened-u-s-health-spending-countries
As always, appreciate your willingness to address challenging issues Joe. This matter is clearly bigger than all of us.
Brian – thanks for the thoughtful comment. I agree with your point about trade-offs, and am trying – with seemingly little success – to get people to understand that our healthcare system is NOT sustainable, and therefore must be replaced with something that is.
Realistically, this will mean lower incomes for physicians, device manufacturers, consultants, and administrators. Longer waits for care, and more difficulty accessing whatever care one desires.
So be it. The alternative is bankruptcy for all of us and our country.
Good post Joe and good discussion. I bring a unique perspective to this discussion as I am from Canada originally. So I have experience as a patient in both systems and a provider in both systems. I have also been involved as a purchaser of health insurance for my company. Firstly, I can tell you that most Canadians love their healthcare system, though, they are taxed more because of it. I believe the stats are 8/10 like it. Even the most conservative folks I know generally like it. Of course there are problems with access for non life threatening conditions. For instance, if you needed a joint replacement you may have to wait 8-10 months.
I did have to bring my father here to see a neurologist because there is a huge shortage of specialists in Canada. He was having some progressive issues that concerned me and he was being told he would need to wait nearly a year for an appointment. Cash buys you the best access to specialists here in the US. I say cash because he was uninsured in the US. Within one week I had him scheduled for an MRI, nerve conduction studies and a consult with a neurologist. Needless to say he was impressed with what a little capitalism can do.
Obviously there are pros and cons to each system. I do have to say that as a provider here Medicare is far easier to deal with and pays providers fairly (debatable and may depend upon the type of provider you are). The private commercial insurance suppliers are not a providers or businesses friend. They have been raising rates to our business all the while cutting what they pay us. Double dipping if you will. And this was going on well before Obamacare. They play both sides of the fence and I can tell you they seem to care nothing about people. I have mixed feelings about having my care in the hands of the government or wall street and fat executives. I believe in capitalism just not sure its principles work well in the health care system? Greed and profits drive the industry and I am not convinced that bodes well when it comes to life and death situations. In addition, if we put more emphasis on prevention and wellness on the front end we could likely save huge $$. If we could just manage chronic conditions that are completely treatable or entirely reversible we would save billions. Neither Medicare or private payers, along with big pharma are really interested. They all give lip service but if we really put money here and incentives you would see innovation.
There has to be a way to blend the good and bad. As Tom well points out we need the money so that we can continue to lead the world in research, treatment and innovation and not sure we get that from a universal or single payer system. Again, perhaps a hybrid type system could be developed that still allowed private payers to provide supplemental benefits? And, maybe even making them run as non profits of some type thereby taking wall street out of the mix. Hopefully we can figure it out because I think we have a real problem and I know we the wealthiest country in the world should be able to figure it out.
Joe,
The Koch Brothers are behind an push to call an Article V Constitutional Convention through their organization, ALEC, the American Legislative Exchange Council. One item they want is a balanced budget amendment which may doom social spending, including single payer, which they oppose as radical libertarians. Add to that what I wrote about recently in Hawaii where Democratic candidates promised voters to support Medicare for All, but told the Healthcare Leadership Council they oppose it and support free market health care. So your prediction may be premature, especially if the SCOTUS enshrines Citizens United into the Constitution. The other thing they want in the Constitution is repeal of the 17th Amendment which directly elects Senators.